Key Takeaways
- Depression in Orange County often co-occurs with alcohol or prescription use, so integrated dual diagnosis care tends to outperform programs that treat each condition on parallel tracks.
- Local options span partial hospitalization, evening IOP for working adults, standard outpatient, and aftercare, letting you match intensity to what your job, commute, and family responsibilities allow.
- Coverage exists across commercial plans protected by federal parity law, Medi-Cal routed through managed care or the county Mental Health Plan, and Medicare for older or disabled residents.2, 11
- Before committing to a program, compare assessment depth, CARF accreditation and DHCS licensure, which evidence-based therapies are actually delivered, step-down planning, and cultural and language fit.
When Depression and Substance Use Show Up Together
If you are reading this while running on fumes, that makes sense. Depression rarely walks in alone. For a lot of people in Orange County, it arrives tangled up with drinking that crept past social, or pills that started as a prescription, or stimulants that kept the workday going until they didn’t. You are not weak for ending up here. You are dealing with two conditions that feed each other.
This is the part most articles about depression treatment options miss. They list therapies and medications as if substance use is a separate problem to handle later. It isn’t. When low mood and substance use overlap, treating one while ignoring the other tends to stall both. Evidence-based care for depression includes psychotherapy, medication, and in some cases brain stimulation, and those tools work best when the substance use piece is in the same room, not down the hall.4
So this guide does two things. It lays out the real range of depression treatment options in Orange County, CA, from partial hospitalization down to weekly outpatient and aftercare. And it stays honest about the dual diagnosis reality, because that is what most working adults, students, and parents in this county are actually facing.
You are looking for a path, not a pitch. The next sections give you one, with the trade-offs named out loud.
Matching Treatment Intensity to What Your Life Allows
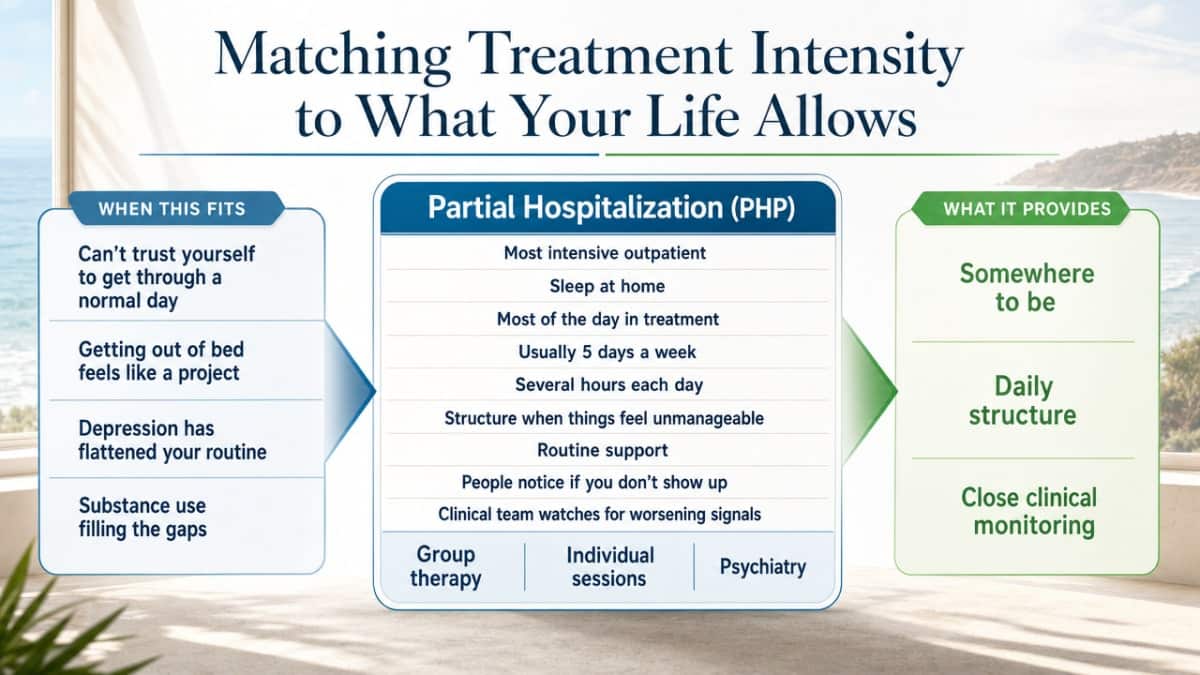
Partial Hospitalization (PHP): Structure When Things Feel Unmanageable
Some weeks, you can’t trust yourself to make it through a normal day. Getting out of bed feels like a project. The drinking or the pills are creeping back, or never really left. That is the territory PHP is built for.
Partial hospitalization is the most intensive option among outpatient depression treatment options in Orange County, CA. You sleep at home, but you spend most of the day in treatment — usually five days a week, several hours each day. That structure matters. When depression has flattened your routine and substance use is filling the gaps, PHP gives you somewhere to be, people who notice when you don’t show up, and a clinical team watching for the signals that things are getting worse.
A typical day blends group therapy, individual sessions, psychiatric check-ins, and skills work. Medication adjustments happen in real time, not three weeks from now. If you are tapering off benzodiazepines or stabilizing on an antidepressant, that close oversight is the point.
PHP is not forever. It is a bridge — usually two to four weeks — designed to get you stable enough to step down without slipping back.
Evening IOP: For People Who Cannot Pause Work or Caregiving
Most adults in Orange County cannot disappear from their lives for a month. You have a job. You have kids who need pickup. You have a partner who is already stretched thin. That reality is exactly why evening intensive outpatient programs exist.
An evening IOP typically runs three to four evenings a week, around three hours per session. You work during the day, handle dinner or homework or whatever the afternoon demands, and then show up for group, individual therapy, and skills practice after hours. It is less intensive than PHP but more structured than a weekly therapy appointment. For depression that co-occurs with substance use, that middle ground is often where the real work happens — close enough to catch a slip, loose enough to let you keep paying rent.
The commute math matters too. The Census Bureau reports that workers age 16+ in Orange County have a mean travel time to work of 26.7 minutes one way.9 Add a daytime treatment program on top of that and you are asking someone to give up the whole day. Evening scheduling removes that obstacle. If you are in Mission Viejo, Irvine, Anaheim, or Santa Ana, you can finish the workday, drive a reasonable distance, and still be home at a decent hour.
This is one of the most underused depression treatment options in Orange County, CA for working adults — partly because people assume real treatment means stepping out of life entirely. It doesn’t have to.
Standard Outpatient and Aftercare: Keeping Gains After the Intensive Phase
Once the worst of it has settled, the question becomes how to hold onto what you have built. Standard outpatient — usually one or two therapy sessions a week, plus a medication check-in every few weeks — is where most people land after PHP or IOP. It is also where some people start, if their depression is moderate and substance use is in early remission or not part of the picture.
Aftercare is the piece a lot of programs skip. It is the structured follow-up that catches you in the months when life looks normal on the outside but the old patterns are still close. Alumni groups, peer support, periodic check-ins with a counselor, occasional family sessions — these are the small touches that keep depression treatment options in Orange County, CA from feeling like a door that closes behind you.
Relapse, for both depression and substance use, often shows up months after intensive treatment ends. That is not failure. It is the nature of the conditions. Aftercare is built to spot the early signals — sleep slipping, isolation, the first drink — before they become another crisis. Staying connected, even loosely, is part of recovery, not an add-on.
Evidence-Based Therapies, Matched to How Depression Actually Presents
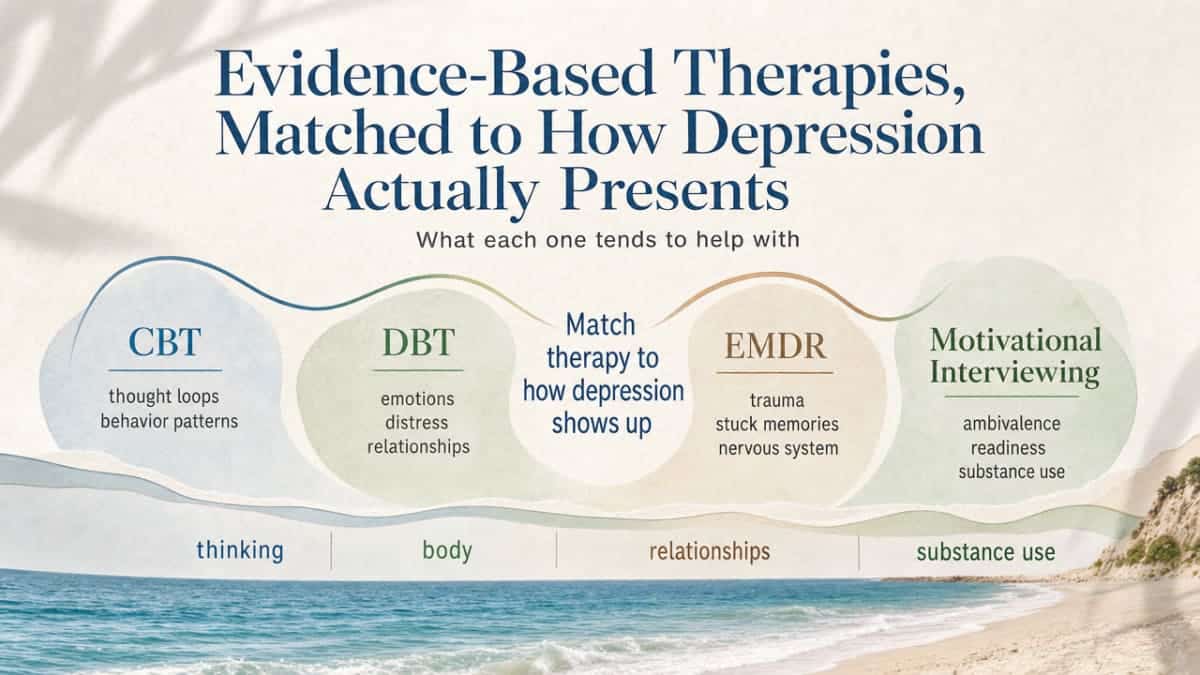
CBT, DBT, EMDR, Motivational Interviewing: What Each One Tends to Help
People talk about therapy like it is one thing. It isn’t. The depression treatment options in Orange County, CA that actually move the needle are the ones matched to how your depression shows up — what it does to your thinking, your body, your relationships, and your use of substances.
Here is a plain-language map of the main evidence-based approaches and what each tends to help with. The National Institute of Mental Health describes psychotherapy, medication, and brain stimulation as the core evidence-based categories for treating depression, with several specific psychotherapies showing strong support.4
- Cognitive Behavioral Therapy (CBT)
- Targets the loops of thought and behavior that keep depression in place. If your inner monologue runs on harsh self-criticism, catastrophic predictions, or the certainty that nothing will help, CBT gives you tools to test those thoughts against reality and rebuild small, repeatable actions. It is one of the most studied psychotherapies for depression.5
- Dialectical Behavior Therapy (DBT)
- Was built for emotion dysregulation — the kind where feelings hit at a 10 and stay there, and where self-harm, impulsive substance use, or relationship blowups follow. If your depression comes with personality disorder features, chronic suicidal thinking, or a pattern of using substances to manage feelings you can’t sit with, DBT’s skills around distress tolerance and emotion regulation tend to fit.
- EMDR (Eye Movement Desensitization and Reprocessing)
- Is for depression that is glued to trauma. When low mood is downstream of something that happened — assault, combat, a childhood you are still carrying — talk therapy alone can spin in circles. EMDR works on the memory itself.
- Motivational Interviewing
- Is less a standalone treatment and more a way of having the conversation when you are unsure whether you want to change at all. With co-occurring substance use, that ambivalence is normal. MI meets it without lectures.
None of these are interchangeable. A good clinician picks based on what you actually bring through the door.
Medication Management and Combined Care
Medication is not a moral question. It is a tool, and for moderate to severe depression, the American Psychological Association’s clinical practice guideline supports psychotherapy, pharmacotherapy, or a combination of the two depending on the person and the severity.6 Combined care — therapy plus medication — is often the strongest path when symptoms are heavy enough to block the work that therapy requires.
What good medication management looks like in practice: a psychiatric provider who takes time to understand your history, including any substance use, and who adjusts based on what is actually happening week to week. Antidepressants do not work the same in every body. The first one prescribed may not be the right one. That is normal, not failure.
For people with co-occurring substance use, this gets more nuanced. Some medications interact poorly with alcohol or other substances. Tapering off benzodiazepines or stabilizing after stimulant use changes what is safe to prescribe and when. This is one of the practical reasons depression treatment options in Orange County, CA work better when psychiatric care lives inside the same program as your therapy — the prescriber sees what the therapist sees, and decisions get made faster.
When Brain Stimulation or Specialty Referrals Enter the Picture
For a smaller group of people, depression does not respond to several rounds of therapy and medication. NIMH lists brain stimulation therapies — including transcranial magnetic stimulation (TMS) and, for the most severe cases, electroconvulsive therapy (ECT) — as evidence-based options when other treatments have not worked.4
These are not first steps. They are specialty referrals, usually made after a careful look at what has been tried and how. Outpatient programs in Orange County typically coordinate these referrals rather than provide them on-site, which is fine — what matters is that someone is watching the full picture and knows when to escalate.
If you have tried multiple medications and therapies without real movement, that is information, not a verdict. The next conversation with your prescriber is about what else exists.
Why Demand for Care in Orange County Has Shifted
Something changed for working adults in California, and the data caught it. A peer-reviewed analysis of California Health Interview Survey responses from 2013 through 2020 found that among employed adults aged 45–65, both depressed mood and suicidal ideation rose by more than 30% in relative terms from 2019 to 2020.12 That is a narrow slice — employed Californians in midlife, measured during the first pandemic year — but it is a real signal, and it lines up with what clinicians in Orange County started hearing in their waiting rooms.
Midlife workers were not supposed to be the headline. The cultural story for years has been about younger adults and teens. But the people picking up the phone to ask about depression treatment options in Orange County, CA shifted too. More were in their late 40s and 50s. More were holding jobs, mortgages, aging parents, and children at the same time. More were quietly using alcohol or prescription medication to keep the wheels turning until the wheels stopped turning.
What that means for you, if you are in that group or love someone who is: the demand pressure is real, but so is the response. Programs have added evening hours. Telehealth options expanded. Depression treatment options in Orange County, CA have grown specifically because midlife workers were not being served by 9-to-5 clinic schedules. If the old model did not fit your life, that was not your failure. The system is catching up.
Paying for Care: Commercial Insurance, Medicare, and Medi-Cal Pathways
Commercial Plans and Mental Health Parity
If you have insurance through your job or the marketplace, the law is on your side in a real way. The Mental Health Parity and Addiction Equity Act requires group health plans and insurers that offer mental health and substance use benefits to apply no stricter limits to those benefits than they apply to medical and surgical care.2 Translation: your plan cannot quietly cap therapy visits or pile on prior authorizations for depression care while leaving knee surgery alone.
What this means when you call a program: ask whether they are in-network with your plan, what level of care your benefits cover (PHP, IOP, outpatient), and whether prior authorization is required. Good programs verify benefits for you before you ever start. Parity does not erase every hurdle — networks vary, and utilization review still happens — but it gives you real ground to stand on if a denial feels off.
Most depression treatment options in Orange County, CA accept the major commercial carriers. Confirm yours before scheduling.
Medi-Cal and the Orange County Mental Health Plan
Medi-Cal covers depression. That is worth saying plainly. The DHCS behavioral health guide notes that Medi-Cal includes coverage for common concerns like anxiety, depression, and stress, plus specialty mental health services for more serious conditions that interfere with daily life.10 California splits responsibility: mild-to-moderate depression typically flows through your Medi-Cal managed care plan, while more severe presentations route through county specialty mental health services.1
In Orange County, the access point for specialty services is the county Mental Health Plan. DHCS publishes the current contact line for Orange County Behavioral Health, which you can call to get screened and connected to programs like intensive outpatient or day treatment for depression.11 That call is the door. It is not a commitment.
If you are unsure which lane you fall into, start with the managed care plan’s behavioral health line on the back of your Medi-Cal card. They will route you. Depression treatment options in Orange County, CA do exist on Medi-Cal — the navigation is the hard part, not the coverage.
Medicare for Older Adults and Some Disabled Residents
If you are on Medicare — whether through age or disability — your depression care is covered more fully than it used to be. Medicare covers outpatient mental health visits, partial hospitalization, screenings, and substance use treatment as part of its mental health benefits.3 That includes the same range of depression treatment options in Orange County, CA that commercial plans cover, just routed differently.
One useful piece of context: a 2025 economic evaluation found that after Medicare cost-sharing parity took effect, beneficiaries with depression used about 0.54 more outpatient mental health visits per year, with a modest increase in average out-of-pocket spending.7 That tells you parity is doing what it was designed to do — more older adults are actually showing up for care.
If you are helping a parent navigate this, ask the program whether they accept Original Medicare or specific Medicare Advantage plans. The answer varies.
Cultural Access and the Latino Community in Orange County
Roughly a third of Orange County is Latino, and the way depression shows up — and gets named — is not the same across every family or every language. For many Spanish-speaking residents, the word for what they are feeling is not depresin. It is exhaustion. It is body pain that does not have a name. It is the sense that something has gone quiet inside.
A community-led intervention developed during the pandemic noted that the disproportionate impact of COVID-19 on Latino communities produced greater reports of depression, anxiety, and stress, and that effective responses had to be culturally grounded rather than clinic-centered.8 That lesson still applies. The depression treatment options in Orange County, CA that work for Latino families tend to be the ones that meet people where they actually are — bilingual clinicians, evening hours that fit shift work, programs that include family rather than treating it as an obstacle, and intake staff who do not flinch at uncertain immigration status. If a program cannot do those things, ask what it can do.
Signals It Is Time to Step Up Your Level of Care
Weekly therapy is enough until it isn’t. Knowing the difference is the part nobody teaches you. Here are the signals that tell you something needs to change — not someday, but soon.
Suicidal thoughts that have a plan, a timeline, or a method. Passive thoughts like “I wish I wasn’t here” are worth telling your therapist about. Thoughts with detail are a reason to call your provider today or reach 988. They are not a personal failing. They are a clinical signal that your current level of care is not holding you.
Substance use that is climbing back, or never stopped. If you are drinking more, using more often, or hiding it from people who would notice, weekly therapy alone is not built for that load. Depression and substance use reinforce each other, and the depression treatment options in Orange County, CA that integrate both — like an IOP or PHP with dual diagnosis expertise — are designed for exactly this moment.
Functional decline you can measure. Missing work. Not showering for days. Letting bills pile up. Sleep that has flipped or collapsed. When the basics start slipping, the structure of a more intensive program is the help that lower levels of care cannot provide. Stepping up is not a setback. It is good clinical judgment.
Choosing a Local Program Without Getting Upsold
Treatment is a service, and like any service, some providers will try to sell you more than you need. Here is how to tell the difference between a program built around your situation and one built around its own census numbers.
Start with the assessment. A good program spends real time understanding what is actually going on — your depression history, any substance use, what you have tried, what your week looks like — before recommending a level of care. If someone tries to admit you to PHP after a ten-minute phone call, that is a flag. The right depression treatment options in Orange County, CA come out of a clinical conversation, not a sales script.
Ask about credentials. Look for CARF accreditation and DHCS licensure, which signal that an outpatient program meets external standards for clinical care. Ask who oversees the clinical work and what their license is. Ask which evidence-based therapies the program actually delivers — CBT, DBT, EMDR, motivational interviewing — versus what shows up on the website but never in the room.5
Frequently Asked Questions
What level of care do I actually need for depression in Orange County?
That answer comes from an honest assessment, not a self-quiz. As a rough guide: weekly outpatient fits mild-to-moderate depression with stable functioning. Evening IOP fits when symptoms are interfering with work or relationships and substance use is in the picture. PHP fits when you cannot reliably take care of yourself. The depression treatment options in Orange County, CA work best when a clinician helps you choose.
Can depression and substance use be treated at the same time?
Yes, and they should be. Treating one while ignoring the other tends to stall both. Integrated dual diagnosis programs handle therapy, medication management, and substance use treatment in the same setting, with one team that sees the full picture. NIMH frames psychotherapy and medication as core evidence-based tools for depression, and those tools work better when substance use is part of the same plan.4
Does insurance cover outpatient depression treatment in Orange County?
Most commercial plans do. Federal parity law requires group health plans and insurers offering mental health benefits to apply limits no stricter than those on medical or surgical care.2That covers outpatient therapy, IOP, and PHP in most cases. Call the program you are considering and ask them to verify benefits before you start. They should tell you what is covered, what needs prior authorization, and where you stand.
How do I access depression treatment if I have Medi-Cal?
Start with the behavioral health number on the back of your Medi-Cal card for mild-to-moderate depression. For more severe symptoms, the county Mental Health Plan handles specialty services like IOP and day treatment, and DHCS publishes the Orange County Behavioral Health contact line.11Medi-Cal covers depression care.10Coverage is not the obstacle. Navigation usually is, so make the call and let them route you.
Which therapy works best for depression — CBT, DBT, or EMDR?
It depends on how your depression shows up. CBT targets thought and behavior patterns. DBT fits emotion dysregulation, chronic suicidal thinking, and substance use as a coping tool. EMDR works when depression is rooted in trauma. NIMH supports several psychotherapies as evidence-based for depression, with the right match depending on the person.4A good clinician picks based on your history, not a default protocol.
When should I step up from weekly therapy to an IOP or PHP?
Step up when the signals get louder: suicidal thoughts that carry a plan or method, substance use that is climbing back, or functional decline you can see in your week — missed work, skipped meals, sleep that has collapsed. The APA guideline supports combined and more intensive care when symptoms are heavier.6Stepping up is not a setback. It is the right clinical move at the right moment.
References
- Mental Health Services Division – DHCS – CA.gov. https://www.dhcs.ca.gov/services/pages/mentalhealthprograms-svcs.aspx
- The Mental Health Parity and Addiction Equity Act (MHPAEA) – CMS. https://www.cms.gov/marketplace/private-health-insurance/mental-health-parity-addiction-equity
- Mental health & substance use disorders – Medicare. https://www.medicare.gov/coverage/mental-health-substance-use-disorder
- Depression – National Institute of Mental Health (NIMH). https://www.nimh.nih.gov/health/topics/depression
- Depression (NIMH Publication). https://www.nimh.nih.gov/health/publications/depression
- Summary of the clinical practice guideline for the treatment of depression across three age cohorts. https://pubmed.ncbi.nlm.nih.gov/34843274/
- Medicare Parity and Outpatient Mental Health Service Use Among Beneficiaries With Depression. https://pmc.ncbi.nlm.nih.gov/articles/PMC12048850/
- Addressing Emotional Wellness During the COVID-19 Pandemic. https://pmc.ncbi.nlm.nih.gov/articles/PMC8220949/
- QuickFacts: Orange County, California. https://www.census.gov/quickfacts/fact/table/orangecountycalifornia/PST045224
- Your Guide to Medi‑Cal Behavioral Health. https://www.dhcs.ca.gov/services/MH/Documents/BH-Brochure-Eng.pdf
- County Mental Health Plan Information – DHCS. https://www.dhcs.ca.gov/individuals/Pages/MHPContactList.aspx
- Increases in Prevalent Depressed Mood and Suicidal Ideation Among Workers During the COVID‑19 Pandemic. https://pmc.ncbi.nlm.nih.gov/articles/PMC9859206/



