Key Takeaways
- Searching for EMDR therapists in Orange County, CA is less about proximity and more about finding a clinician whose training, pacing, and trauma expertise match what your nervous system actually needs.
- EMDR holds the strongest recommendation in major PTSD treatment guidelines, with weekly 90-minute sessions over about three months for single-incident trauma and longer arcs for complex cases 2.
- Trauma and substance use travel together — past-year PTSD reached 10.0% in addiction medicine departments — so dual-diagnosis fluency and dissociation screening matter when vetting local clinicians 3.
- Before booking, compare EMDRIA training versus certification, recovery experience, pacing philosophy, evening availability, and how each therapist coordinates with psychiatrists, sponsors, or DBT and VA providers.
What you’re actually looking for when you search for an EMDR therapist
When you type “EMDR therapists in Orange County, CA” into a search bar, you’re rarely looking for a list. You’re looking for someone who can hold the work — someone who understands that trauma lives in the body, that your nervous system has its own timeline, and that healing doesn’t move in a straight line. That search itself is a step forward, even if it doesn’t feel like one yet.
Maybe you’ve already done talk therapy. Maybe you’ve sat in groups, taken medication, worked a program, and still find that certain memories hijack your week. That’s not failure on your part. It’s information. It tells you the next step probably needs to reach the parts of memory that words alone can’t quite touch — which is exactly what Eye Movement Desensitization and Reprocessing was built to do.2
So as you read on, think of this less as a directory and more as a vetting guide. The right EMDR therapist isn’t always the closest one. They’re the one whose training, pacing, and comfort with co-occurring conditions match what your recovery actually needs. Among EMDR therapists in Orange County, CA, that fit matters more than the freeway exit. You deserve a clinician who can meet you where your nervous system is — not where a treatment manual assumes you should be.
Why EMDR earned its place as a first-line PTSD treatment
EMDR didn’t start as a household name. It started in 1987 as a clinical observation, then spent three decades being tested, doubted, refined, and tested again. What pulled it from the fringe to the front of major treatment guidelines wasn’t marketing — it was outcome data that kept holding up. The VA National Center for PTSD now lists EMDR with the strongest possible recommendation across several major clinical practice guidelines for PTSD, putting it on equal footing with the most established trauma-focused therapies.2
That standing matters when you’re choosing among EMDR therapists in Orange County, CA. It means you’re not picking an alternative or experimental approach. You’re picking a treatment that the VA, the Department of Defense, and international guideline bodies have independently landed on after reviewing the same evidence.2
The session structure is part of why it works in real life. EMDR is typically delivered weekly, in sessions that can run up to 90 minutes, over roughly three months for single-incident trauma.2That’s a real container — long enough for your nervous system to settle into the work, short enough that you can see an endpoint from where you’re sitting today. For complex trauma layered with addiction or other mental health conditions, the arc usually stretches longer, and a careful clinician will tell you that upfront.
A 2024 narrative review of EMDR trials found that more than two-thirds of the studies it examined showed significant PTSD improvement, while honestly noting that some trials used waitlist controls or modest sample sizes.1That mix — strong signal, with methodological humility — is exactly the posture you want from EMDR therapists in Orange County, CA. The evidence is real. It’s also still being sharpened. A clinician who can hold both truths is one worth a consultation call.
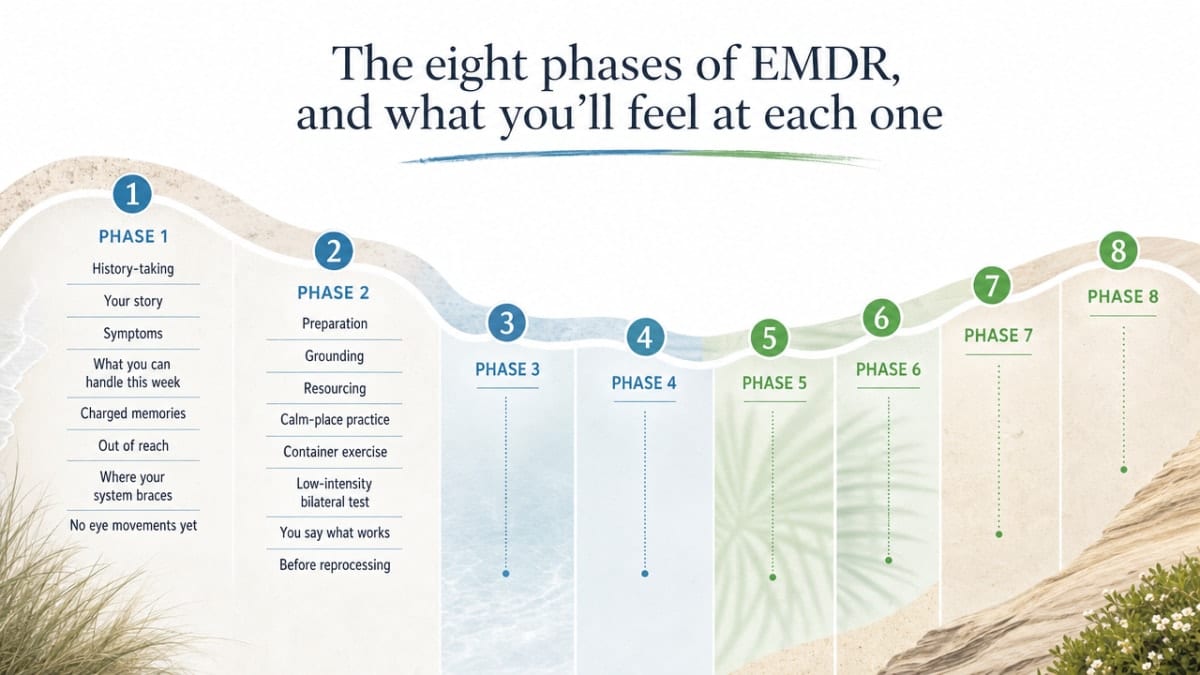
The eight phases of EMDR, and what you’ll feel at each one
Phases 1-2: History-taking and preparation
The first sessions don’t involve any eye movements, tappers, or light bars. They involve a conversation — sometimes a long one — about your story, your symptoms, and what you can already handle in a given week. Good EMDR therapists in Orange County, CA treat this stretch as the foundation, not the warm-up. They’re listening for which memories feel charged, which ones feel out of reach, and where your nervous system tends to brace.
In Phase 2, your clinician teaches you grounding and resourcing skills before any reprocessing begins. You might practice a calm-place visualization, learn container exercises for what you’re not ready to open yet, or test bilateral stimulation at low intensity just to see how your body responds.2You get to say what works and what doesn’t. That’s not a side note — it’s the work.
If you’ve felt rushed by past therapists, this phase can feel almost too slow. It’s not. Trauma taught you to scan for safety, and Phase 2 is where you build the actual evidence that this room, this person, and these tools can hold you. You’ll know you’re ready for Phase 3 when you’ve used your resources successfully between sessions, not just inside one.
Phases 3-6: Assessment, desensitization, installation, body scan
Phase 3 is where you and your therapist pick a specific target — usually a single image, the worst moment of a memory, or a body sensation that keeps surfacing. You’ll identify the negative belief attached to it (“I’m powerless,” “It was my fault”) and the positive belief you’d rather hold instead. You’ll rate how true each one feels and how disturbing the memory is right now, on simple scales. It can feel clinical. It’s actually a map.2
Phase 4 is desensitization — the part most people picture when they imagine EMDR. You hold the target in mind while your therapist guides bilateral stimulation: eye movements, alternating taps, or auditory tones. Then you pause. You notice what came up: an image, a sensation, a memory you hadn’t thought about in years, sometimes nothing at all. There’s no script for what’s supposed to happen. Your job is to notice and report. Your therapist’s job is to keep you in the window where the memory is accessible but not overwhelming.
Phase 5 installs the positive belief you chose in Phase 3, pairing it with bilateral stimulation until it starts to feel earned rather than rehearsed. Phase 6 is a body scan — you bring the original memory back to mind and notice where, if anywhere, your body still holds tension. If something lights up, you reprocess it. If nothing does, that’s data too.2
The full eight-phase protocol — History-Taking, Preparation, Assessment, Desensitization, Installation, Body Scan, Closure, and Reevaluation — is the framework every EMDRIA-trained clinician follows, and it’s documented by the VA National Center for PTSD as the standard structure of the therapy.2Knowing the map helps you stay oriented when the territory gets uneven.
Phases 7-8: Closure and reevaluation
Phase 7 closes each session, whether the memory is fully reprocessed or not. Your therapist helps you return to a stable baseline before you walk out the door — back to your calm place, back into your body, back into the version of you that can drive home. If the work felt unfinished, that’s normal. Closure is not the same as completion. It’s a deliberate pause that respects how reprocessing keeps unfolding between sessions, often in dreams or quiet moments.2
Phase 8 happens at the start of your next session. You and your therapist check in on what shifted, what surfaced, and whether the original target still carries the same charge. Sometimes a memory that felt like a 9 last week registers as a 3. Sometimes a new layer appears. Either way, you decide together what to target next.
This rhythm — open, reprocess, close, return — is what makes EMDR therapists in Orange County, CA more like steady companions than performers. The protocol is structured. Your pace inside it is yours.
Why EMDR matters when trauma and substance use travel together
If you’re in recovery and still carrying trauma, you already know they don’t stay in separate lanes. A flashback can light up a craving. A craving can pull you back toward the very thing your nervous system was trying to mute in the first place. This loop isn’t a character flaw — it’s a wiring problem that talk therapy alone often can’t fully reach. That’s part of why EMDR therapists in Orange County, CA who understand addiction recovery are worth the extra effort to find.
That comorbidity is exactly why EMDR has earned attention in recovery-aware care. A meta-analysis of EMDR trials found that the therapy reduces not only PTSD symptoms but also the depression and anxiety that so often ride alongside trauma — and alongside early sobriety.6When the trauma quiets, the secondary symptoms that have been driving so much of your daily distress often quiet with it.
The honest caveat: a systematic review of EMDR in adults with co-occurring substance use disorders found promising signals but also acknowledged that the trials are still small and uneven in quality.7So EMDR isn’t a guarantee. It’s a well-supported tool that becomes more powerful when the clinician holding it understands cravings, relapse cycles, and the way shame compounds trauma. When you’re calling EMDR therapists in Orange County, CA, ask directly whether they’ve worked with people in active recovery. The ones who hesitate are telling you something useful. The ones who say yes — and can describe how they’d coordinate with your other providers — are the ones worth your first session.

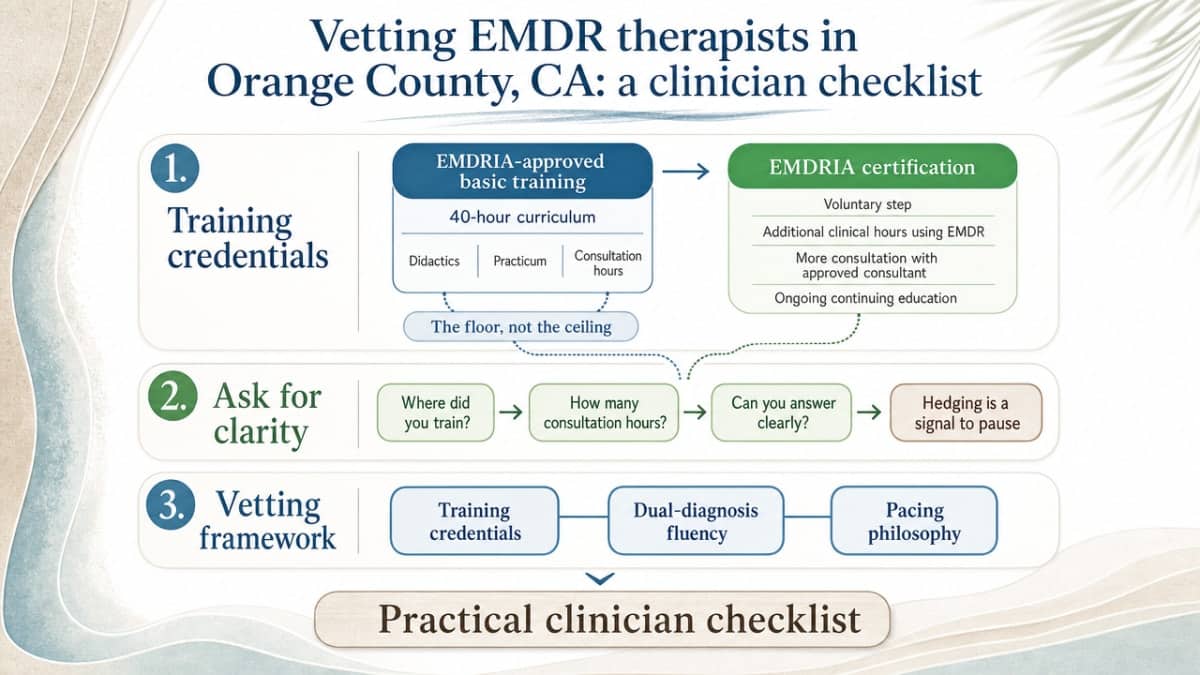
Vetting EMDR therapists in Orange County, CA: a clinician checklist
EMDRIA basic training vs. certification
Not every clinician who lists EMDR on their website has the same training behind it. The first question to ask is whether they completed an EMDRIA-approved basic training — the standard 40-hour curriculum that includes didactics, practicum, and consultation hours. That’s the floor, not the ceiling.
EMDRIA certification is a separate, voluntary step. Certified therapists have logged additional clinical hours using EMDR, completed more consultation with an approved consultant, and earned ongoing continuing education in the model. Among EMDR therapists in Orange County, CA, you’ll find both — and either can do excellent work. What matters is that they can answer the question clearly. If a clinician hedges about where they trained or how many consultation hours they’ve completed, that hesitation is data. A trained therapist will name their training program, their consultant, and roughly how many EMDR cases they’ve carried. You’re allowed to ask. Trauma survivors who ask better questions tend to land with better fits.
Dual-diagnosis fluency and dissociation screening
If you’re in recovery, the second question is whether your therapist actually works with people like you. EMDR in a vacuum is different from EMDR delivered alongside cravings, sponsor calls, medication-assisted treatment, and the daily work of staying sober. A 2024 review of EMDR research noted that while the therapy is highly efficacious overall, methodology and population matter — outcomes are strongest when clinicians are matched to the complexity in front of them.1
Ask directly: “Have you treated people with co-occurring substance use? How do you handle a session when a craving comes up afterward?” Listen for specifics, not reassurance. A clinician who’s done this work will mention coordinating with your psychiatrist, pacing reprocessing around early sobriety, or pausing if dissociation rises.
Dissociation screening is the other non-negotiable. Trauma sometimes teaches the brain to leave the room — to float, blank out, or feel unreal under stress. EMDR therapists in Orange County, CA who are trained for complex trauma will screen for dissociation before any reprocessing begins, often using a brief written measure. If no one has ever asked you about these experiences, that’s a sign you may need a clinician with more trauma-specific depth.
Pacing, consultation, and the right to slow down
The last filter is the one most directories skip: how does this clinician handle pace? EMDR moves fast when it works — and the fastest-working therapy is not always the right one for a nervous system that’s been carrying weight for decades. You want a therapist who treats slowing down as part of the protocol, not a sign you’re failing it.
Ask whether they use a consultant or consultation group. Even seasoned EMDR therapists in Orange County, CA bring complex cases to peer consultation; it’s a sign of clinical maturity, not inexperience. Ask what they do when a session opens more material than can be closed in 90 minutes. Ask how they’d respond if you said, “I need to pause reprocessing for a few weeks and just stabilize.”
The answers will tell you whether this person sees you as a partner in the work or a case to move through. You have the right to slow down. A good therapist will already know that.
When EMDR is not the right starting point
Here’s something most therapy pages won’t tell you: sometimes the most caring thing a clinician can do is delay EMDR. Not refuse it. Delay it. The protocol is powerful precisely because it opens trauma material — and if your nervous system or daily life can’t hold what opens, reprocessing can leave you more dysregulated than before. Honest EMDR therapists in Orange County, CA will tell you this on the first call.
Active withdrawal is one clear pause point. If your body is still detoxing from alcohol, benzodiazepines, or opioids, you don’t have the physiological stability to track a memory, your therapist’s hand, and your own breath at the same time. Medical stabilization comes first, then a stretch of sober days before Phase 3 begins. A 2024 review of EMDR research stressed that outcomes depend heavily on whether clinicians match the protocol to the complexity in front of them.1
Unmanaged dissociation is another. If you regularly lose time, feel outside your body for hours, or can’t tell where one part of you ends and another begins, you need stabilization and dissociation-specific work before reprocessing. Acute psychosis, active suicidality, and an unsafe living situation all sit in the same category — real reasons to pause, not to disqualify.
The right starting point in these moments is often Phase 2 work that never quite ends: resourcing, grounding, building a relationship with a therapist who can hold the long view. That’s not failing at EMDR. That’s how it actually begins.
How EMDR fits with sobriety, 12-step, DBT, and medication
EMDR doesn’t ask you to put the rest of your recovery on hold. It works best when it lives inside the support you’ve already built. If you’re going to meetings, your sponsor relationship stays. If you’re in a DBT skills group, those skills become part of your between-session toolkit. If you’re on medication managed by a psychiatrist, that continues — and ideally, your providers talk to each other.
Twelve-step work and EMDR don’t compete. The fellowship gives you community, accountability, and a place to talk about cravings out loud. EMDR works on the older material underneath the cravings — the moments your body learned to brace, run, or numb. Many people in recovery find that as trauma reprocesses, the white-knuckle quality of early sobriety softens. That’s not a replacement for the steps. It’s the rooms getting a little easier to sit in.
DBT and EMDR pair especially well. The distress tolerance and emotion regulation skills you’ve practiced in DBT become the resourcing your EMDR therapist leans on in Phase 2 and Phase 7. Skilled EMDR therapists in Orange County, CA will ask what DBT skills you already use and weave them in by name.
Medication is part of the picture too. EMDR is a psychotherapy, and major guidelines recommend psychotherapy over medication alone for PTSD because the gains tend to be larger and last longer.4That doesn’t mean stopping your prescriptions. It means your psychiatrist and your EMDR therapist are working the same case from different angles. Ask your therapist how they coordinate with prescribers. The answer should be specific, not vague.
Access in Orange County: referrals, evening hours, and veteran pathways
Finding the right clinician is one thing. Actually getting in the door is another. Most people searching for EMDR therapists in Orange County, CA hit the same three walls: psychiatry waitlists, a 9-to-5 schedule that doesn’t bend for therapy, and a referral path that feels like guesswork.
The most direct entry is usually through your existing care team. If you’re already seeing a psychiatrist, a primary care doctor, or an addiction medicine clinician, ask them for a warm handoff to a trauma-focused therapist. PTSD prevalence has been climbing in integrated behavioral health settings — one analysis tracked a rise from 24.6% of adult behavioral health patients in early 2019 to 31.6% by late 2022, with disproportionate impact on women and LGBTQIA+ patients.9Your provider has likely referred others recently and knows who actually takes new clients.
If you’re working full-time or raising kids, evening hours aren’t a luxury — they’re the difference between starting EMDR and putting it off another year. When you call EMDR therapists in Orange County, CA, ask about evening slots and whether they protect those hours for established clients. Some clinicians reserve late afternoons specifically for working adults in recovery.
For veterans, the VA pathway is its own door. EMDR sits alongside Cognitive Processing Therapy and Prolonged Exposure as a recommended first-line trauma therapy in the VA/DoD 2023 guideline, so you can ask your VA provider directly for an EMDR referral — either inside the VA or through community care.4You don’t have to settle for whichever therapist is assigned first if EMDR is what your nervous system is asking for.
A soft place to start when you’re ready
You’ve read this far, which means some part of you is already moving toward this work. That counts. The search for EMDR therapists in Orange County, CA isn’t a transaction — it’s a decision your nervous system gets to weigh in on, one call at a time.
When you’re ready, start with two or three consultation calls. Ask about EMDRIA training, dual-diagnosis experience, and pacing. Notice who listens, who answers plainly, and who doesn’t rush you off the phone. For trauma survivors looking for integrated outpatient care alongside EMDR therapists in Orange County, CA, 449 Recovery in Mission Viejo is one option worth knowing about. Whatever you choose, the next small step is enough.
Frequently Asked Questions
How do I know if an EMDR therapist in Orange County, CA is properly trained?
Ask where they completed their EMDRIA-approved basic training, who their consultant was, and roughly how many EMDR cases they’ve carried. Certified EMDR therapists in Orange County, CA have logged additional clinical hours and ongoing consultation beyond basic training. A trained clinician will answer plainly — hesitation about credentials is itself useful information for you.
How long does EMDR therapy usually take to work?
For single-incident trauma, EMDR is often delivered weekly in sessions up to 90 minutes over about three months.2Complex trauma layered with addiction or other mental health conditions typically takes longer. A careful clinician will tell you upfront that pacing depends on your nervous system, your stability, and how much preparation work Phase 2 needs before reprocessing begins.
Can I do EMDR if I’m still early in recovery from substance use?
Often yes, with the right clinician and timing. Active withdrawal is a pause point — your body needs medical stabilization first. Once you have some sober days behind you, EMDR therapists in Orange County, CA who understand recovery can pace reprocessing around cravings and coordinate with your other providers. A systematic review found promising signals for EMDR in this population, though evidence is still maturing.7
Will EMDR make me relive my trauma in detail?
No. EMDR is not exposure therapy. You don’t narrate the memory in detail or stay inside it. You hold a brief image or sensation in mind while your therapist guides bilateral stimulation, then pause and notice what comes up. You stay in the present, in the room, with your eyes open. If something becomes overwhelming, you pause. You stay in charge.
Does EMDR help with depression and anxiety, or only PTSD?
It often helps with both. A meta-analysis of EMDR trials found significant improvements not only in PTSD symptoms but also in comorbid depression and anxiety compared with control conditions.6When the underlying trauma quiets, the secondary symptoms that have been driving daily distress often soften alongside it. That’s part of why EMDR matters for trauma survivors carrying layered diagnoses.
Can I continue 12-step meetings, DBT, or medication while doing EMDR?
Yes — and you should. EMDR works best inside the support you’ve already built. Your sponsor relationship, DBT skills group, and psychiatrist all stay in place. Skilled EMDR therapists in Orange County, CA actively coordinate with prescribers and weave your existing DBT skills into resourcing and closure phases. Ask any therapist you’re considering how they communicate with the rest of your care team.
References
- Revisiting Eye Movement Desensitization and Reprocessing Therapy: A Narrative Review. https://pmc.ncbi.nlm.nih.gov/articles/PMC11111257/
- Eye Movement Desensitization and Reprocessing (EMDR) for PTSD. https://www.ptsd.va.gov/professional/treat/txessentials/emdr_pro.asp
- Prevalence and Health Care Utilization of Posttraumatic Stress Disorder and Trauma-Related Disorders. https://pmc.ncbi.nlm.nih.gov/articles/PMC12485246/
- VA/DoD 2023 Clinical Practice Guideline for the Management of PTSD. https://www.ptsd.va.gov/professional/treat/txessentials/cpg_ptsd_management.asp
- Posttraumatic Stress Disorder and Acute Stress Disorder (ACOEM Guideline excerpt in MTUS). https://www.dir.ca.gov/dwc/dwcpropregs/MTUS-Evidence-Based-Update/Guidelines/ACOEM-PTSD-Guideline.pdf
- The effectiveness of EMDR therapy for PTSD and comorbid disorders: A meta-analysis. https://pubmed.ncbi.nlm.nih.gov/34894137/
- Efficacy of EMDR in reducing trauma-related symptoms in adults with substance use disorders: A systematic review. https://pubmed.ncbi.nlm.nih.gov/32267048/
- Management of Posttraumatic Stress Disorder and Acute Stress Disorder. https://www.healthquality.va.gov/guidelines/mh/ptsd/
- Examining PTSD Prevalence Among Underserved Populations in Primary Care Integrated Behavioral Health Settings. https://pmc.ncbi.nlm.nih.gov/articles/PMC11555738/
- Hospital and Workforce Behavioral Health Data in California – HCAI. https://www.hcai.ca.gov/data/initiatives/behavioral-health/



