Key Takeaways
- Substance use and mental health conditions often fuel each other, which is why integrated drug addiction treatment addresses both at once instead of in sequence 1, 3.
- Concurrent care delivered by one team produces better outcomes for substance use, psychiatric stability, and daily functioning than fragmented or parallel approaches 5.
- Evidence-based programs match therapy to the specific dual diagnosis — CBT, DBT, trauma-focused work, motivational interviewing, contingency management — with medication and family involvement as supporting tools 4, 7.
- Look for outpatient integrated care that assesses both conditions at intake, coordinates therapy and prescribing on one team, and builds aftercare from day one 2, 10.
The Loop You’re Already Living In
If you’re reading this late at night, or between shifts, or after another argument that ended with a door closing — you already know the shape of it. The anxiety shows up first. Or the depression. Or the flashback, the racing thoughts, the heaviness that makes ordinary days feel impossible. So you reach for something that takes the edge off. A drink. A pill. A line. Whatever quiets the noise.
And it works. For a little while.
Then it stops working. The thing that helped you sleep starts wrecking your sleep. The thing that calmed your panic starts feeding it. Your mental health symptoms come back louder, and the substance you used to manage them is now its own problem. So you use more. And the loop tightens.
This is not a character flaw. It’s one of the most common patterns in mental health care, and clinicians have a name for it: co-occurring disorders. Federal guidance from SAMHSA describes how substance use and mental health conditions frequently coexist and shape each other, which is exactly why integrated drug addiction treatment exists in the first place 1. You are not failing at recovery. You are caught in a system that was, until recently, often treated in two separate rooms by two separate teams who didn’t talk to each other.
The good news — and there is good news — is that the room has changed.
What Co-Occurring Actually Means (and Why It’s More Common Than You Think)
A co-occurring disorder is just clinical shorthand for what you’re probably already living: a substance use disorder and a mental health condition happening in the same body, at the same time, shaping each other. SAMHSA defines it broadly on purpose — any combination of two or more substance use and mental disorders can co-occur, which means there’s no single picture of what a person with dual diagnosis looks like 2.
It could be panic attacks and a nightly bottle of wine. PTSD from something you’ve never told anyone about and a benzodiazepine prescription that stopped being enough. ADHD that went undiagnosed until your twenties and stimulants that started feeling like the only way to keep up. Bipolar episodes you tried to flatten with alcohol. Depression you tried to outrun with cocaine. The specific pairing matters clinically, but the underlying pattern is the same — two conditions, one nervous system, constant interaction.
And it’s not rare. SAMHSA describes co-occurring disorders as common enough that integrated drug addiction treatment is the recommended approach, not a niche specialty 1. NIDA puts it plainly: when a substance use disorder shows up alongside another health condition, it is usually better to treat them at the same time rather than separately 3.
Here’s what that means for you. If you’ve ever been told to “get sober first, then we’ll deal with your mental health,” or to “stabilize your mental health first, then we can talk about the drinking” — that’s an older model of care, and the research has moved past it. Clinicians who work in dual diagnosis are trained to look at both at once, because trying to untangle them in sequence usually means one condition flares while you’re focused on the other 8. You weren’t imagining the loop. The loop is the whole point.
Why Treating One Without the Other Rarely Holds
Integrated vs. Sequential vs. Parallel Care
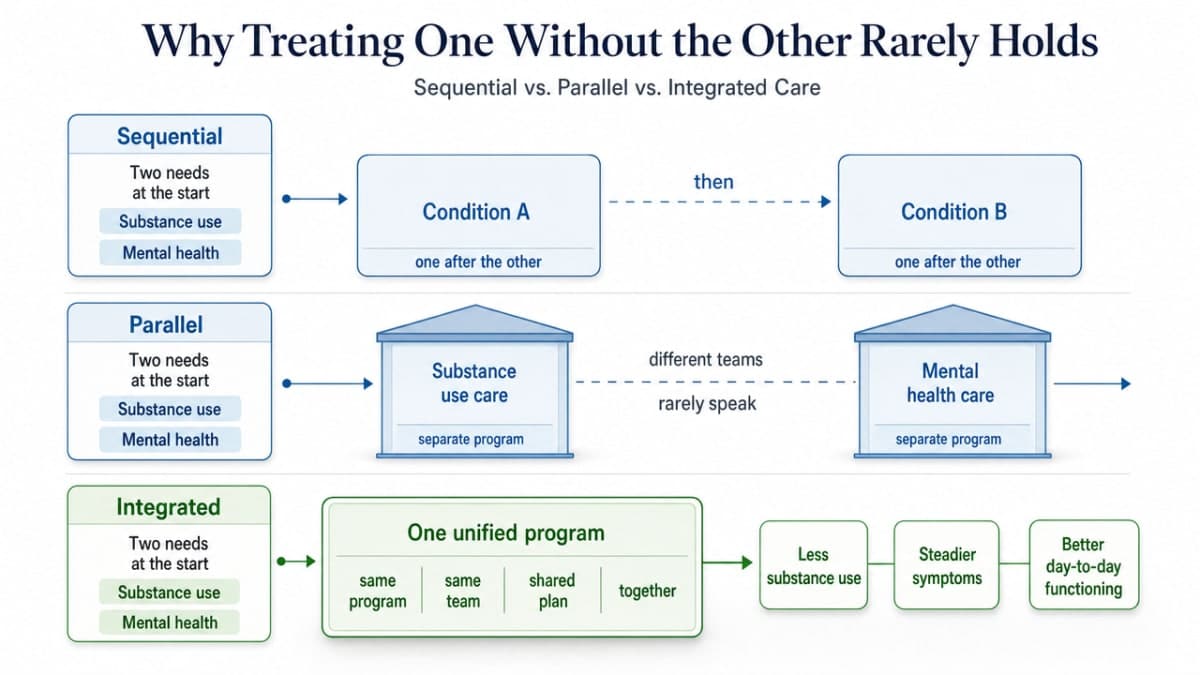
There are really three ways a system can respond when you walk in with both a substance use disorder and a mental health condition:
- It can treat them one after the other (sequential).
- It can treat them at the same time, but in two different buildings, with two different teams who rarely speak (parallel).
- Or it can treat them together, in the same program, by the same team, with one shared plan. That last one is integrated care — and it’s the one the evidence keeps pointing to.
A peer-reviewed review of integrated treatment for co-occurring disorders found that when the same provider or team addresses both conditions concurrently, people see better outcomes across three domains that probably matter most to you right now: substance use goes down, psychiatric symptoms get steadier, and day-to-day functioning improves 5. Compare that to fragmented care, where you’re often left translating between your therapist and your prescriber, or worse, repeating the hardest parts of your story to strangers who don’t have the full picture.
SAMHSA backs this up at the policy level, describing integrated assessment and treatment as the preferred response to dual diagnosis rather than two parallel tracks that may never meet 2. The model exists because the loop you’re living in doesn’t respect appointment calendars. Your symptoms don’t wait their turn, so your drug addiction treatment shouldn’t either.
The Standard of Care, Not an Upgrade
Here’s something worth sitting with: integrated drug addiction treatment is not a luxury tier. It’s not the deluxe version that only some people qualify for. It’s what the major federal agencies say should happen when someone shows up with both conditions.
NIDA’s position is direct — when a substance use disorder occurs alongside another health condition, it is usually better to treat them at the same time rather than separately 3. NIMH frames integrated care as the model that combines mental health and substance use treatment into one coordinated plan, supported by behavioral therapies and, when appropriate, medication 4. SAMHSA has gone as far as building an Integrated Treatment for Co-Occurring Disorders KIT to help providers actually put this into practice 10.
What Integrated Drug Addiction Treatment Actually Looks Like
The Assessment That Sees Both at Once
The first real difference shows up in the intake. In a single-condition program, you’d answer questions about your substance use, full stop. In integrated drug addiction treatment, the same clinician asks about both — what you’re using, how often, what it does for you, and also when the anxiety started, how the depression moves through your week, whether you’ve ever been diagnosed with PTSD, ADHD, OCD, or something nobody quite named.
That dual lens is on purpose. SAMHSA’s guidance is built around the idea that any combination of substance use and mental health conditions can co-occur, so the assessment has to be wide enough to catch them together rather than label one and ignore the other 2. Clinicians trained in dual diagnosis are looking for the overlaps you’ve probably already noticed yourself — the way the drinking spikes when the panic spikes, the way the stimulant use tracks with the depressive crashes 8.
You will be asked questions that feel personal fast. Sleep. Trauma history. Family. Medications you’ve tried and stopped. What a bad day looks like. None of it is filler. Each answer shapes the treatment plan, because the plan only works if it accounts for both conditions at once. If an assessment doesn’t ask about your mental health, that’s a signal you’re in the wrong room.
Matching Therapy to the Condition You’re Carrying
Once the assessment is done, the next question is what kind of therapy actually fits what you’re living with. This is where drug addiction treatment stops being a single product and starts being a set of evidence-based tools matched to the specific shape of your dual diagnosis. NIMH names several of the therapies that show up most often in integrated care, and each one has a job 4.
If anxiety or depression is the mental health half of the picture, cognitive behavioral therapy is usually somewhere in the plan. CBT teaches you to notice the thoughts that fuel the spiral and to interrupt them before they hand you a reason to use. It’s structured, it’s practical, and it tends to be one of the first tools introduced because it works on both sides of the loop 4.
If trauma is underneath the substance use — and for a lot of people, it is — trauma-focused therapy is the lane. Approaches like EMDR and other trauma-focused work give you a way to process what happened without re-traumatizing yourself, which matters because untreated PTSD is one of the most common drivers of relapse.
If your nervous system runs hot, if emotions feel like they arrive at full volume with no warning, dialectical behavior therapy is often the better fit. DBT was built originally for people with emotion dysregulation and personality disorders, and it teaches concrete skills — distress tolerance, emotion regulation, interpersonal effectiveness — that translate directly into the moments when you’d otherwise reach for a substance.
If you’re ambivalent about change — not sure you want to stop, not sure you can, not sure what life looks like on the other side — motivational interviewing meets you there. It doesn’t push. It helps you find your own reasons 4.
And for stimulant use specifically, contingency management — a structured behavioral approach that reinforces non-use — has one of the strongest evidence bases NIMH names 4. Group therapy and family-based interventions wrap around all of it, because addiction doesn’t happen in isolation and recovery doesn’t either 4. You don’t have to memorize the acronyms. You just have to know that the right drug addiction treatment program will match the therapy to your condition, not hand everyone the same worksheet.
Medication’s Real Role in Dual Diagnosis
Medication in integrated drug addiction treatment is not about replacing one substance with another, and it’s not the centerpiece. It’s one tool on a team that includes therapy, peer support, and the relationships you’re rebuilding. But when it’s used well, it can take enough pressure off the nervous system to let the rest of the work happen.
NIMH describes medications as part of the integrated care toolkit for co-occurring conditions, used alongside behavioral therapies rather than instead of them 4. Some medications can address symptoms across more than one disorder at the same time, which matters when your mental health and substance use are tangled together 7. A prescriber working in dual diagnosis is thinking about both — what helps the depression without raising relapse risk, what stabilizes mood without dulling the therapy you’re doing, what supports a careful taper off a benzodiazepine or opioid without leaving you white-knuckling withdrawal alone.
For people with more complex presentations, including serious mental illness alongside substance use, treatment guidelines specifically recommend pairing pharmacotherapy with psychosocial interventions rather than relying on either alone 6. That pairing is the point. The medication isn’t supposed to do everything. It’s supposed to make everything else reachable. If your prescriber and your therapist are on the same team and talking to each other, that’s integrated drug addiction treatment doing what it’s designed to do.
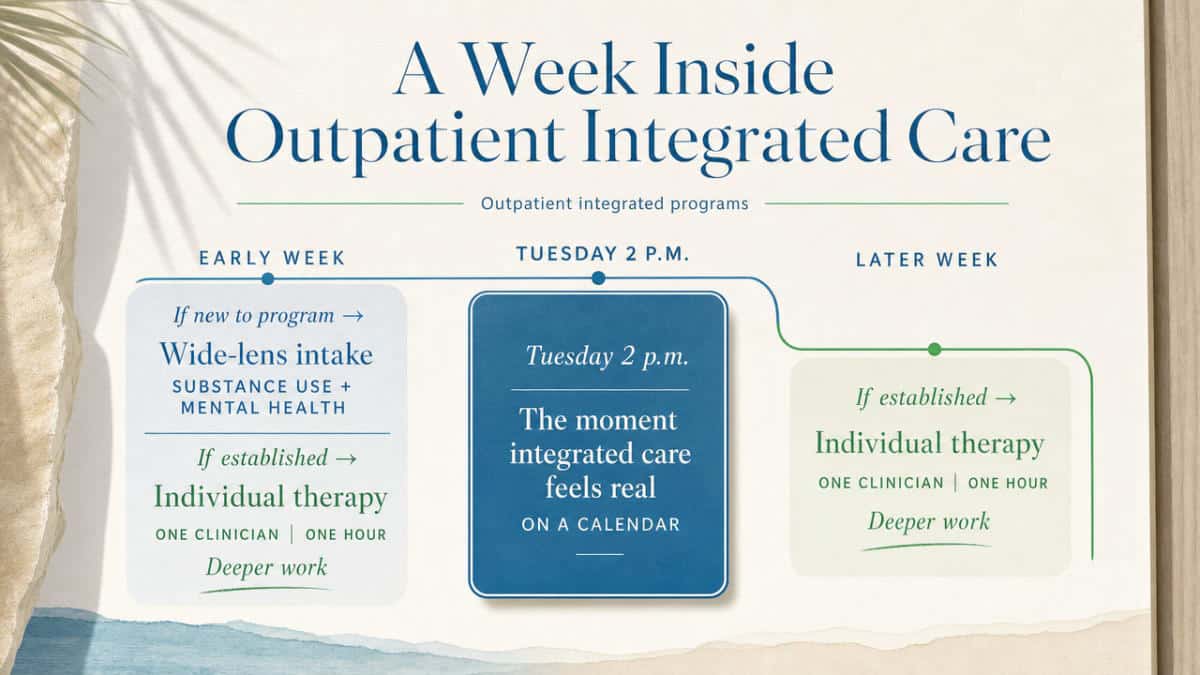
A Week Inside Outpatient Integrated Care
One of the most useful things you can do before starting drug addiction treatment is picture the actual week. Not the brochure version. The Tuesday-at-2-p.m. version. Because the abstract idea of “integrated care” only starts to feel real when you can see where it lives on a calendar.
Here’s the shape it tends to take in outpatient integrated programs, drawing on the model NIMH and SAMHSA describe for co-occurring conditions 4, 1.
Early in the week, if you’re new to the program, you sit for the dual assessment — the wide-lens intake that asks about both your substance use and your mental health in the same conversation 2. If you’re already established, the week usually opens with an individual therapy session. One clinician. One hour. The space where the deeper work happens — the trauma, the relationships, the specific reasons the substance kept feeling necessary.
Midweek brings group therapy, often more than once. Group is where you stop being the only person in the room who knows the loop from the inside. It’s also where skills get rehearsed — DBT skills, CBT tools, relapse prevention strategies — in a setting that mirrors real life better than any one-on-one can 4.
A family session lands somewhere in the week when it’s appropriate. NIMH names family-based interventions as part of evidence-based integrated care for a reason — the people who live with you are part of the recovery environment whether they’re in the room or not 4.
Psychiatric and medication review happens on its own cadence, usually weekly or biweekly early on, then less often as things stabilize. The prescriber checks how medications are landing, adjusts as needed, and stays in contact with your therapy team so the plan moves as one piece 7.
Aftercare and peer support aren’t bolted on at the end — they thread through the week from the beginning. Alumni groups, 12-step or alternative meetings, case management check-ins. The point is that drug addiction treatment is building the scaffolding you’ll lean on after the program intensity steps down.
That’s a week. It’s a lot, and also — and this matters — it’s designed to fit around the rest of your life, not replace it.
Keeping Your Job, Your Family, and Your Treatment
One of the quietest fears about starting drug addiction treatment is the one nobody puts on a form: If I do this, will I lose everything I’m still holding together? The job. The kids’ school pickup. The lease. The version of yourself your family still recognizes.
That fear is reasonable. It’s also one of the main reasons outpatient integrated care exists. You don’t have to disappear from your life to get well. SAMHSA’s framing of integrated care for co-occurring disorders is built around person-centered, recovery-oriented services that meet people where they actually live — work, family, community — rather than pulling them out of all of it 1. NIMH describes integrated treatment the same way: mental health and substance use care coordinated into one plan, designed to be sustainable alongside the rest of your responsibilities 4.
In practice, this looks like a schedule you can hold. Daytime programming for people whose evenings belong to their kids. Evening intensive outpatient for people whose paychecks depend on showing up to a 9-to-5. Family sessions that bring the people you love into the room instead of leaving them outside the conversation 4. A treatment team that knows you’re going to have a hard Tuesday and plans for it.
Your family is part of this too — not as a problem to manage, but as a recovery environment. When the people closest to you understand the loop, they stop accidentally feeding it. That’s why family-based interventions are baked into evidence-based drug addiction treatment, not tacked on as an extra 4.
You don’t have to choose between getting help and keeping your life. The whole point of integrated outpatient care is that those two things were never supposed to be separate.
When the Picture Is More Complex: Bipolar, Psychosis, and Serious Mental Illness
Not every dual diagnosis fits a neat shape. If what you’re carrying includes bipolar disorder, schizoaffective disorder, or another serious mental illness alongside a substance use disorder, you’ve probably already discovered that the loop gets louder and the stakes get higher. Manic episodes can pull you toward stimulants or alcohol. Depressive crashes can pull you toward anything that quiets them. Psychotic symptoms can make ordinary triggers feel unbearable. And the medications that help your mental health can interact in real ways with the substances you’re trying to stop using.
This is exactly the population integrated drug addiction treatment was designed to hold. Treatment guidelines for people with substance use disorders and serious mental illness are clear that concurrent care — pharmacotherapy paired with psychosocial interventions, delivered by a team that talks to itself — outperforms anything that tries to handle the conditions in isolation 6. A psychiatrist who knows you’re working a relapse prevention plan prescribes differently than one who doesn’t. A therapist who knows your bipolar diagnosis adjusts the work when a mood episode arrives instead of treating it like a setback.
If you’ve been turned away from programs because your mental health was “too complex,” or sent to mental health programs that wouldn’t touch the substance use, that’s a signal — not about you, but about the program’s scope. Integrated drug addiction treatment for serious mental illness exists, and the guidelines say it’s what should happen 6.
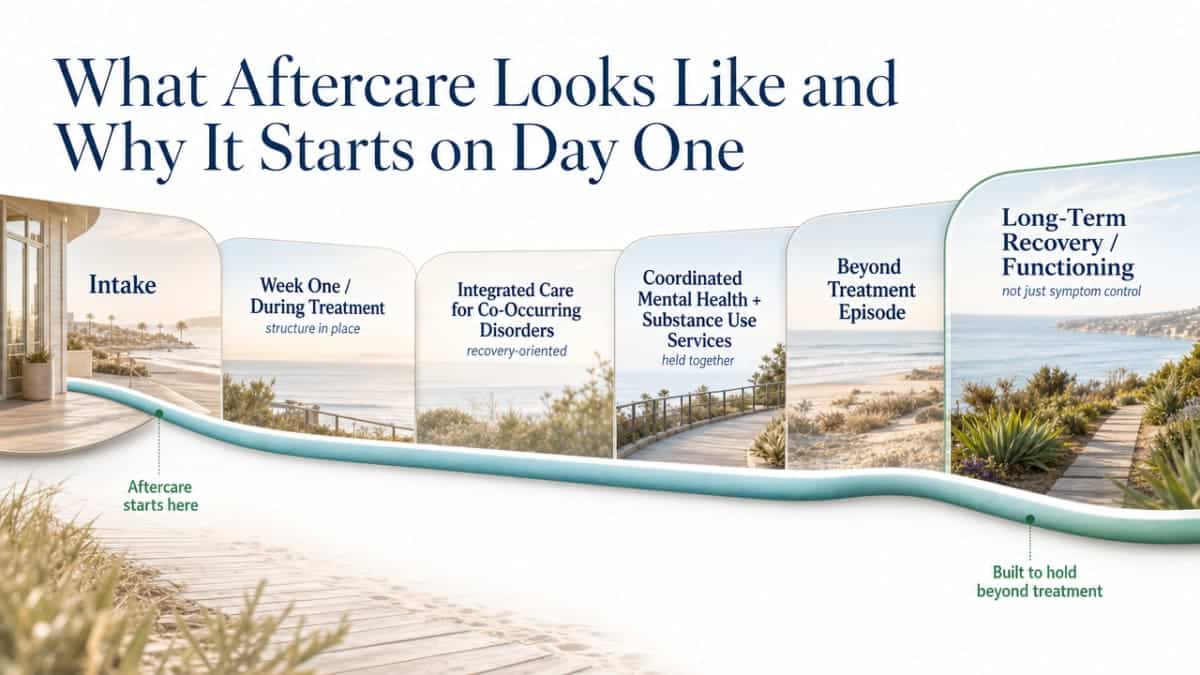
What Aftercare Looks Like and Why It Starts on Day One
Aftercare is one of those words that sounds like an ending. It’s actually a beginning that’s been quietly running in the background since your intake.
Good drug addiction treatment programs start building the after-version of your life from week one — not because the program is short, but because the work you do during treatment only sticks if there’s a structure waiting on the other side of it. SAMHSA’s framing of integrated care for co-occurring disorders is explicitly recovery-oriented, which means the plan is pointed at long-term functioning, not just symptom control during the program 1. The Integrated Treatment for Co-Occurring Disorders KIT was built to help providers do exactly this — coordinate mental health and substance use services in a way that holds beyond the treatment episode 10.
In practice, aftercare looks like a step-down. The intensity of programming eases. The therapy continues, often weekly. Psychiatric and medication check-ins keep going on a longer cadence. Alumni groups and peer support meetings become the steady weekly anchors. Family members who were in sessions with you stay part of the plan.
Taking the Next Step Without Doing It Alone
If you’ve read this far, something in you is already moving. That counts.
The hardest part of starting drug addiction treatment is rarely the treatment itself. It’s the phone call before the treatment. The moment where you have to say out loud, to a stranger, what you’ve been carrying quietly. You don’t have to have the right words. You don’t have to know which program, which therapy, which diagnosis. You just have to make contact with someone trained to take it from there.
SAMHSA runs a National Helpline that’s free, confidential, and open 24 hours a day, every day of the year. It connects people with local treatment options, including programs that handle co-occurring conditions 9. If you’re in Orange County and looking specifically for outpatient integrated care that treats mental health and substance use together — the kind of program 449 Recovery was built around — that call, or one to a local dual diagnosis provider, is a real first step.
The loop you’ve been living in is not the end of the story. Integrated drug addiction treatment exists for exactly this reason, and you don’t have to walk into it alone.
Frequently Asked Questions
Can drug addiction treatment really address my mental health at the same time?
Yes — and that’s exactly what integrated drug addiction treatment is designed to do. SAMHSA and NIDA both recommend treating substance use and mental health conditions at the same time, by the same team, rather than in sequence 1, 3. Concurrent care is associated with better outcomes across substance use, psychiatric stability, and daily functioning compared to fragmented treatment 5.
How do I know if I have a co-occurring disorder versus just one condition?
A proper dual diagnosis assessment is the only honest answer. SAMHSA defines co-occurring disorders broadly — any combination of substance use and mental health conditions can qualify 2. If your symptoms get worse when you stop using, or your use spikes when symptoms flare, that pattern is worth screening. Clinicians trained in dual diagnosis use structured assessment to identify both conditions rather than labeling one 8.
What types of therapy are used in integrated drug addiction treatment?
NIMH names several evidence-based therapies used in integrated care: cognitive behavioral therapy for anxiety and depression, trauma-focused approaches for PTSD, dialectical behavior therapy for emotion dysregulation, motivational interviewing for ambivalence, and contingency management for stimulant use 4. Family-based interventions are part of the model too 4. The right mix depends on your specific dual diagnosis, not a one-size formula.
Can I keep working and stay with my family while in treatment?
Outpatient integrated care is built for exactly this. SAMHSA describes integrated treatment as person-centered and recovery-oriented, designed to fit into your real life rather than pull you out of it 1. Evening intensive outpatient schedules, daytime programming, and family sessions all exist so you can keep your job, your relationships, and your treatment on the same calendar 4.
Will I have to take medication for both my mental health and substance use?
Not necessarily. Medication is one tool, not the centerpiece. NIMH describes medications as part of the integrated toolkit used alongside behavioral therapies 4. Some medications can address symptoms across more than one condition at once 7. For people with serious mental illness alongside substance use, guidelines recommend pairing pharmacotherapy with psychosocial care 6. Your prescriber decides with you, not for you.
Where can I turn if I’m not sure where to start?
SAMHSA’s National Helpline is free, confidential, and open 24 hours a day, every day of the year. It connects callers to local treatment resources, including programs that handle co-occurring conditions 9. You don’t need a diagnosis, a plan, or the right words. You just need to make the call — or reach out to a local dual diagnosis provider — and let someone trained take it from there.
References
- Managing Life with Co-Occurring Disorders. https://www.samhsa.gov/mental-health/serious-mental-illness/co-occurring-disorders
- Co-Occurring Disorders and Other Health Conditions. https://www.samhsa.gov/substance-use/treatment/co-occurring-disorders
- Co-Occurring Disorders and Health Conditions. https://nida.nih.gov/research-topics/co-occurring-disorders-health-conditions
- Finding Help for Co-Occurring Substance Use and Mental Disorders. https://www.nimh.nih.gov/health/topics/substance-use-and-mental-health
- Integrating Treatment for Co-Occurring Mental Health Conditions. https://pmc.ncbi.nlm.nih.gov/articles/PMC6799972/
- Treatment Guidelines for Substance Use Disorders and Serious Mental Illness. https://pmc.ncbi.nlm.nih.gov/articles/PMC3285548/
- Substance Use and Co-Occurring Mental Disorders. https://hicares.hawaii.gov/2023/06/substance-use-and-co-occuring-mental-disorders/
- Simplified Clinician Guidelines for Treatment of Co-Occurring Disorders. https://library.immaculata.edu/Dissertation/Psych/Psyd449TaylorTroutA2021.pdf
- National Helpline. https://www.samhsa.gov/find-help/helplines/national-helpline
- Co-Occurring Disorders Materials Available. https://radarcart.boisestate.edu/library/files/2017/07/CoOccurringDisordersResourceMaterials1.pdf



