Key Takeaways
- Among treatment centers in Orange County, CA, the label ‘dual diagnosis’ is common, but only integrated models place mental health and substance use under one team, one assessment, and one treatment plan 6, 8.
- California’s oversight splits between DHCS mental health divisions and the Drug Medi-Cal Organized Delivery System, and parallel-track care tends to hide in the gaps between those two regimes 2, 3.
- Before referring, verify the legal entity, license type, and licensed address through DHCS, and ask intake who writes the treatment plan and how the prescriber and therapist actually coordinate 11.
- Compare programs on PHP, IOP, and aftercare availability, evening track access, language match for the client, and whether relapse is treated as clinical data rather than grounds for discharge 10.
Reading the Signal: What Separates Integrated Dual Diagnosis Care From the Rest
If you’re triaging a placement for someone with co-occurring conditions, you already know the hardest part isn’t finding a program. It’s finding one that actually treats both diagnoses as a single clinical picture. Among treatment centers in Orange County, CA, the marketing language tends to flatten that distinction — “dual diagnosis” appears on nearly every landing page, but the underlying care model can range from genuinely integrated to two separate tracks running in parallel, occasionally meeting at a shared lunch table.
That gap matters. SAMHSA’s guidance is direct: integrated treatment, where the same clinical team addresses mental health and substance use together, produces better outcomes than parallel or sequential models — including reduced substance use and meaningful improvement in psychiatric symptoms and functioning 6. Peer-reviewed reviews of co-occurring disorders reach the same conclusion, with the added caveat that implementation varies widely across programs that all describe themselves the same way 8.
So when you’re reading a website, an intake packet, or a discharge plan, you’re looking for structural signals, not adjectives. Is there one treatment plan or two? Does the psychiatric prescriber communicate with the substance use counselor in real time, or by fax three weeks later? Is screening for both conditions built into the front door, or is one condition treated as the “real” problem and the other as a complication?
The rest of this guide gives you a working frame for answering those questions across treatment centers in Orange County, CA — grounded in DHCS oversight, evidence-based practice, and the questions that quickly separate genuine integration from co-located services.
The Orange County Behavioral Health Landscape You’re Actually Navigating
How California Structures Oversight: DHCS, DMC-ODS, and What Counties Must Arrange
Before you compare treatment centers in Orange County, CA, it helps to know who’s actually watching the watchers. The California Department of Health Care Services (DHCS) sits at the top of the behavioral health oversight chain. Its Medi-Cal Behavioral Health Policy Division shapes both Specialty Mental Health Services and the Drug Medi-Cal program, which means the same agency is setting expectations for the mental health and substance use sides of dual diagnosis care 2.
The Drug Medi-Cal Organized Delivery System (DMC-ODS) is where that policy meets the street. It defines the levels of substance use disorder care counties must arrange for eligible members, sets quality standards, and operates a statewide non-emergency referral line that supplements local pathways 3. Orange County participates in DMC-ODS, which is why you’ll see consistent language around ASAM levels and care coordination requirements across many programs here — even programs that primarily serve commercial insurance still tend to align their clinical framework with these standards.
On the mental health side, the picture is broader. The DHCS Mental Health Services Division oversees publicly funded programs spanning children, adults, and older adults, plus the Office of the Ombudsman that handles beneficiary concerns 1. For your purposes as a referrer, two practical implications follow. First, when a program markets itself as treating co-occurring conditions, it sits at the intersection of two oversight regimes that don’t always speak the same dialect. Second, the gaps between those regimes are exactly where parallel-track care tends to hide. A program can be properly licensed for substance use services and offer mental health counseling on the side without ever functioning as a truly integrated dual diagnosis program. Knowing which agency governs which service helps you ask sharper questions about how the two are actually woven together inside the building.
Local Entry Points: The OC 24/7 Access Line and Crisis System Intersections
When the placement question is urgent, you have more entry points than the average referral pad suggests. DHCS maintains a directory of every county’s 24/7 substance use disorder access line, and Orange County’s line is listed with a continuously staffed phone number and a county SUD website that includes a provider directory 4. For someone in active crisis or a family member trying to figure out where to start at 2 a.m., that line is often the fastest way into a coordinated triage conversation rather than a guessing game.
The crisis side of the system has its own touchpoints. The Orange County Sheriff’s Behavioral Health Bureau pairs law enforcement response with behavioral health outreach, focusing on people experiencing homelessness and people with mental health needs who interact with patrol 5. You won’t route a stable IOP candidate through the Sheriff’s Bureau, but you should know it exists, because clients with co-occurring conditions sometimes touch this system before they touch yours. A solid outpatient program will have a working relationship with these crisis touchpoints and a clear plan for what happens when a client decompensates between sessions.
The practical map looks like this: the county access line and crisis teams function as front doors. Outpatient treatment centers in Orange County, CA function as the longer-term clinical home. The handoff between them is where good programs distinguish themselves — by accepting warm referrals, by communicating with county case managers, and by responding within hours rather than days when a partner agency calls. Ask any program you’re vetting how often they take referrals directly from the county access line and how those handoffs work in practice.
Demographic Context: Who Programs in Orange County Are Built to Serve
Orange County is not a monolith, and the treatment centers in Orange County, CA that serve it well don’t pretend otherwise. Census QuickFacts data show a county with substantial racial and ethnic diversity and a wide income spread across cities and unincorporated areas 7. That demographic reality has direct clinical consequences: language access, cultural framing of mental health, family involvement norms, and the willingness to engage with formal services all vary across the communities a program serves.
For you as a placement decision-maker, this changes the vetting conversation. A program that can deliver evidence-based therapy in English but has no bilingual clinician available for a Spanish-dominant client is not a viable match for that client, no matter how strong its DBT or trauma protocols look on paper. The same logic applies to Vietnamese-speaking clients, Farsi-speaking clients, and the many other language communities that make up the county.
Population-based mental health estimates for California counties come largely from the California Health Interview Survey, which is designed to produce county-level mental health indicators across demographic groups 14. The takeaway isn’t a single statistic to recite — it’s that need is distributed unevenly across the county, and the programs worth shortlisting can speak specifically about which communities they serve well and where their gaps are. If a program can’t answer that question honestly, that’s information too.
Integrated vs. Parallel vs. Sequential: The Clinical Distinction That Matters Most
Why ‘No Wrong Door’ Is a Structural Claim, Not a Marketing Slogan
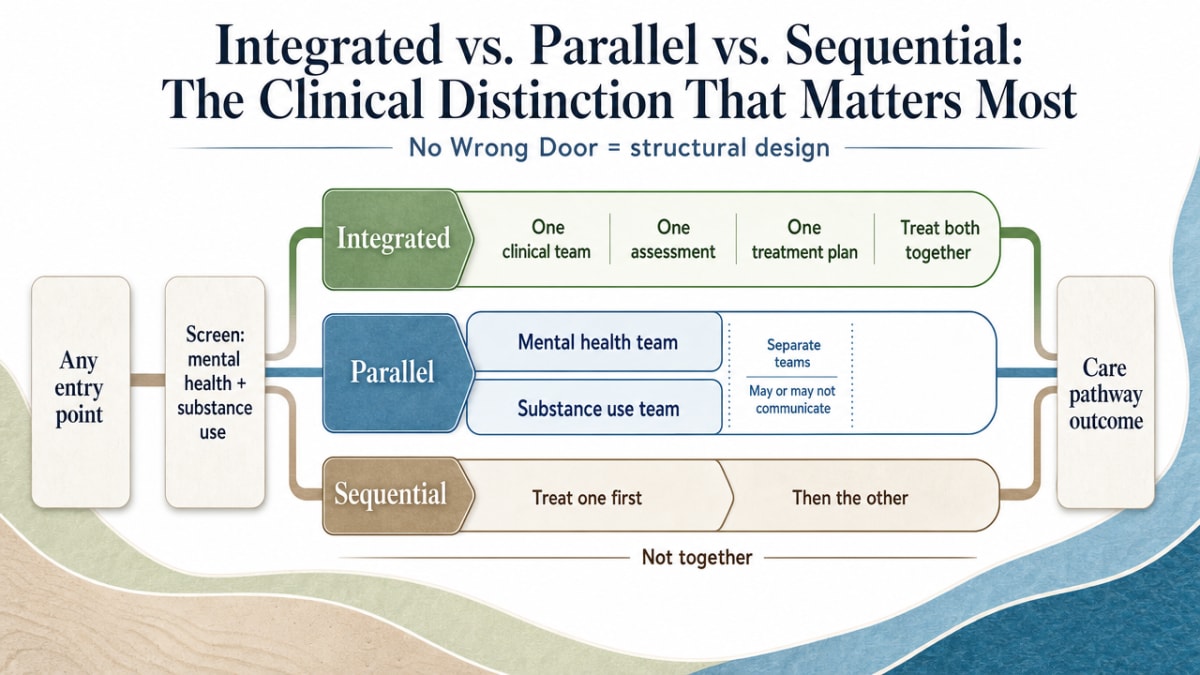
You’ve probably heard “no wrong door” used as a tagline. It’s actually a structural commitment. SAMHSA’s framing is that any entry point into the behavioral health system should screen for both mental health and substance use conditions and route the person into care that treats both together — not bounce them between agencies until one finally takes the case 6. That’s a design standard, not a brochure line.
The three models you’re sorting between look like this in practice. Integrated care places mental health and substance use treatment under one clinical team, one assessment, and one treatment plan. Parallel care delivers both services at the same time but through separate teams that may or may not communicate. Sequential care treats one condition first — usually the substance use — and only addresses the other after some milestone is reached. Peer-reviewed reviews of co-occurring care consistently find that integrated models produce better engagement, stronger reductions in substance use, and more meaningful improvement in psychiatric symptoms than parallel or sequential approaches, with the caveat that programs labeled “integrated” vary widely in how fully they implement the model 8.
That variability is the part you have to read for. When you’re vetting treatment centers in Orange County, CA, ask who writes the treatment plan, who attends case conference, and how often the prescriber and the primary therapist actually talk about a shared client. If those answers point to one team holding both diagnoses at once, you’re looking at integration. If they point to two teams with a shared waiting room, you’re looking at parallel care wearing an integrated label.
Sequencing, Medication Complexity, and What Evidence-Based Actually Looks Like
Integration isn’t a single protocol — it’s a clinical posture toward a hard problem. Reviews of substance use disorder care with co-occurring depression, anxiety, and ADHD show that sequencing decisions matter and that medication management often gets more complicated, not less, when both conditions are on the table at the same time 10. A stimulant prescription for ADHD reads differently when the client also has a stimulant use history. An SSRI started in week one looks different from one started after thirty days of stabilization. These are clinical judgment calls, and they require a team that can hold the whole picture.
What you want to hear from a program is specificity. Which evidence-based therapies do they actually deliver, by whom, and with what fidelity? Cognitive behavioral therapy, dialectical behavior therapy, motivational interviewing, and trauma-focused approaches like EMDR all have a research base for co-occurring populations, but a program that lists every modality on its website without naming who’s certified in what is often signaling marketing reach rather than clinical depth.
The medication conversation is a useful stress test. Ask how the psychiatric prescriber coordinates with the substance use counselor when a client’s symptoms shift. Ask how they handle a client who arrives on benzodiazepines and needs a medically supervised taper while also working on trauma. Ask what happens when a client relapses mid-treatment — is the response a clinical recalibration or a discharge?
Programs that can answer those questions in plain language, without retreating to slogans, are demonstrating the kind of integrated thinking the evidence base actually calls for. Among treatment centers in Orange County, CA, that’s the distinction worth shortlisting on.
Levels of Care: PHP, IOP, and the Step-Down That Supports Reintegration
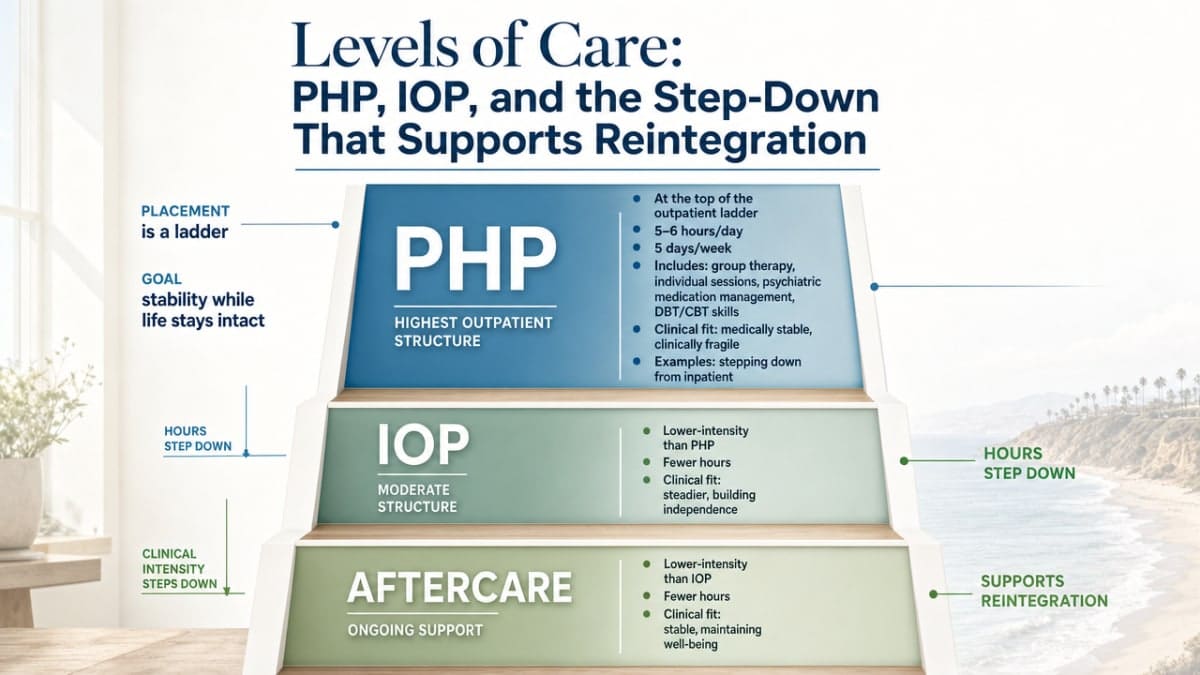
Placement isn’t a single decision — it’s a ladder. The question isn’t just “does this client need treatment,” but “which rung gets them stable while keeping the rest of their life intact?” The DMC-ODS framework structures substance use care into defined levels, and most treatment centers in Orange County, CA that handle co-occurring conditions organize their outpatient programs along the same logic 3.
Partial hospitalization (PHP) sits at the top of the outpatient ladder. You’re looking at roughly five to six hours of structured clinical contact, five days a week — group therapy, individual sessions, psychiatric medication management, and skills work like DBT or CBT delivered in concentrated blocks. PHP fits the client who is medically stable but clinically fragile: someone stepping down from inpatient, someone whose symptoms are too active for weekly outpatient, or someone whose home environment can hold them overnight but not all day.
Intensive outpatient (IOP) drops the dose without dropping the structure. Typical IOP runs nine to fifteen hours per week across three to five sessions, and the evening tracks that several treatment centers in Orange County, CA now offer are often the difference between a client engaging in care and dropping out to keep a job. For a working parent or a graduate student, an evening IOP isn’t a convenience feature — it’s the only level of care that respects the rest of their life.
Aftercare is where the ladder either holds or breaks. Weekly groups, alumni programming, continued individual therapy, medication follow-up, and warm handoffs to community supports turn a discharge into a transition. Programs that treat aftercare as an afterthought tend to lose clients in the first sixty days post-discharge, which is exactly when relapse risk is highest for co-occurring populations 10.
When you’re matching acuity to setting across treatment centers in Orange County, CA, the questions are concrete. Can the client tolerate full days of clinical work without destabilizing? Do they have a safe place to sleep? Are they medically stable enough that a higher level of care isn’t safer? And critically — does the program you’re considering actually offer the step-down rungs, or will your client hit a cliff at week six because there’s no IOP or aftercare to land on?
Verifying a Program Is What It Says It Is
DHCS License Lookup and What Counts as a Licensable Service
The fastest way to separate marketing from reality is to check the license. DHCS requires facilities providing alcohol and other drug (AOD) recovery or treatment services — including detoxification, individual and group counseling sessions, and educational programming — to hold the appropriate license or certification, and the Licensing and Certification Division maintains the records you can verify against 11. If a program describes itself as offering substance use treatment but you can’t find a corresponding license, that’s not a paperwork gap. That’s a clinical risk.
The mental health side works differently. Many outpatient programs don’t require the same facility licensure that governs higher-acuity settings like Mental Health Rehabilitation Centers or Psychiatric Health Facilities, which fall under the DHCS Mental Health Licensing and Certification Branch 12. That doesn’t mean outpatient mental health services run unregulated — individual clinicians hold their own board licenses, and programs that prescribe operate under medical oversight — but it does mean that for treatment centers in Orange County, CA offering dual diagnosis care, the substance use components are typically the licensable piece on the facility side.
What you want to confirm for any program on your shortlist: the legal entity name (not just the marketing name), the license type and number, the specific services authorized under that license, and whether the address you’re routing clients to matches the licensed address. A program operating multiple sites should be able to tell you which site is licensed for what. If intake can’t answer those questions in one phone call, you’ve already learned something about how the program runs.
The Complaint Pathway and What It Reveals About Accountability
The complaint pathway is worth knowing about before you need it. DHCS investigates complaints against licensed and certified AOD treatment programs and against registered or certified counselors, with intake channels that include an online form, fax, and mail 13. The same guidance clarifies that sober living environments providing licensable services can also be investigated — which matters when a treatment program is paired with affiliated housing that markets itself as part of the clinical experience.
For you as a referrer, two practical uses follow. First, when something feels off about how a program is handling a client — abrupt discharge, medication mismanagement, billing that doesn’t match the level of care delivered — there’s a formal channel, and using it generates a record. Second, the existence of that channel is a question you can ask programs directly. A center that talks openly about its complaint history, regulatory inspections, and what it changed in response is signaling a different culture than one that gets defensive. You’re not looking for a spotless record. You’re looking for accountability.
Intake Questions That Quickly Separate Integrated From Co-Located
A fifteen-minute intake call will tell you most of what you need to know if you ask the right questions. Skip the brochure topics and go straight to structure.
Who writes the treatment plan, and is there one plan or two? In a genuinely integrated program, mental health and substance use goals sit in a single document maintained by a single team. Two plans is parallel care.
How often does the psychiatric prescriber communicate with the primary therapist about a shared client? Real answers sound like “weekly case conference, plus direct messaging in the EHR.” Marketing answers sound like “we have great communication.”
What happens when a client relapses during treatment? Programs aligned with the evidence base treat relapse as clinical information that recalibrates the plan, not as grounds for discharge 10. If the answer is administrative — “we’d have to step them up” without clinical detail — the dual diagnosis label may be thinner than it appears.
How do you screen for both conditions at the front door? SAMHSA’s “no wrong door” standard means any entry point screens for both mental health and substance use 6. Programs that screen for one and refer out for the other are running parallel care.
Which evidence-based therapies do you deliver, by whom, with what certification? Specificity here separates clinical depth from modality bingo. Across treatment centers in Orange County, CA, the programs worth shortlisting answer these questions in plain language, without retreating to slogans.

Red Flags Worth Acting On
Most warning signs at treatment centers in Orange County, CA aren’t dramatic. They’re small inconsistencies that add up. Here are the ones worth slowing down for.
Intake can’t name the license. If the person on the phone can’t tell you the legal entity, license type, and licensed address for substance use services, the program may be operating outside the oversight DHCS expects 11. Verify before you refer.
Two separate plans, two separate teams. If the psychiatric side and the substance use side maintain different treatment plans and rarely meet, you’re looking at parallel care wearing a dual diagnosis label 6.
Relapse triggers administrative discharge. Programs aligned with the evidence treat relapse as clinical data, not a rule violation 10. A quick step to discharge tells you how the program actually thinks about co-occurring conditions.
Affiliated housing with vague boundaries. If a program pairs with sober living that delivers what sound like licensable services without clear oversight, DHCS can investigate — and so should you 13.
Modality bingo without named clinicians. Long lists of therapies with no one certified to deliver them is marketing depth, not clinical depth. Across treatment centers in Orange County, CA, specificity is the signal.
Making the Placement Decision
You’ve done the work. You’ve read past the marketing language, asked the structural questions, and watched how intake responds when you push past the brochure. Now you’re choosing between two or three treatment centers in Orange County, CA that all look defensible on paper. Here’s how to close the decision.
Match the client, not the average. The right placement for a working parent with anxiety and an alcohol use disorder isn’t the right placement for a graduate student with bipolar II and a benzodiazepine taper ahead of them. Evening IOP availability, prescriber depth, DBT fidelity, and language access matter differently in each case. Let the client’s clinical picture set the weight on each factor.
Trust what you heard on the phone. Programs that answered your structural questions in plain language — one treatment plan, weekly case conference, relapse as clinical data 10— are showing you their actual practice. Programs that retreated to slogans showed you that too.
If the placement is right, the next call you make is to the program. If you want a starting point built around integrated outpatient dual diagnosis care, 449 Recovery in Mission Viejo is one of the treatment centers in Orange County, CA worth that call.
Frequently Asked Questions
How do I verify that a program is actually licensed to provide the services it advertises?
Ask intake for the legal entity name, license type, license number, and licensed address, then confirm those details against the DHCS Licensing and Certification records 11. Services like detoxification, counseling sessions, and educational programming trigger licensure requirements on the substance use side. If the marketing name and licensed entity don’t match, or intake can’t answer in one call, treat that as a clinical risk worth resolving before you refer.
What’s the practical difference between integrated, parallel, and sequential dual diagnosis care?
Integrated care puts mental health and substance use under one team, one assessment, one treatment plan. Parallel care delivers both at once but through separate teams that may not communicate. Sequential care treats one condition first, then the other. Among treatment centers in Orange County, CA, integrated models produce better engagement and stronger improvement in psychiatric symptoms and substance use outcomes than parallel or sequential approaches 6, 8.
When should I route someone to the OC 24/7 access line versus directly to an outpatient program?
Use the Orange County 24/7 SUD access line when the situation is urgent, ambiguous, or after hours, or when the person needs coordinated triage and a provider directory rather than a single program 4. Go direct to an outpatient program when you’ve already assessed acuity, identified a clinical match among treatment centers in Orange County, CA, and need to schedule intake. The two pathways complement each other.
What intake questions quickly reveal whether a program offers true integrated care?
Ask who writes the treatment plan and whether there’s one plan or two. Ask how often the prescriber and primary therapist communicate about shared clients. Ask how front-door screening handles both conditions, in line with SAMHSA’s no-wrong-door standard 6. Ask what happens clinically when a client relapses mid-treatment. Specific, plain-language answers signal integration. Slogans, vague reassurances, or administrative responses signal parallel care wearing a dual diagnosis label.
How do PHP, IOP, and aftercare fit together when placing a client with co-occurring conditions?
Partial hospitalization fits clients who are medically stable but clinically fragile, needing concentrated daily structure. Intensive outpatient (including evening tracks) lowers intensity while preserving work and family responsibilities. Aftercare holds the gains through alumni groups, continued therapy, and medication follow-up. The DMC-ODS framework structures these levels across treatment centers in Orange County, CA 3. Match acuity to setting, and confirm the program offers each rung so your client doesn’t hit a cliff.
What should I do if I have concerns about how a treatment center is operating?
Document specifics — dates, names, what happened clinically — then file a complaint through DHCS, which investigates licensed and certified AOD programs and certified counselors through online, fax, and mail channels 13. The same pathway covers affiliated sober living that delivers licensable services without oversight. Filing creates a record regulators can act on and helps you make more informed referrals to treatment centers in Orange County, CA going forward.
References
- Mental Health Services Division – DHCS. https://www.dhcs.ca.gov/services/pages/mentalhealthprograms-svcs.aspx
- Behavioral Health Services – DHCS. https://www.dhcs.ca.gov/services/Pages/BHS.aspx
- Drug Medi-Cal Organized Delivery System – DHCS. https://www.dhcs.ca.gov/provgovpart/Pages/Drug-Medi-Cal-Organized-Delivery-System.aspx
- SUD County Access Lines – DHCS. https://www.dhcs.ca.gov/individuals/Pages/sud_county_access_lines.aspx
- Behavioral Health Bureau | Orange County California. https://www.ocsheriff.gov/commands-divisions/patrol-operations-command/southwest-operations/behavioral-health-bureau
- Managing Life with Co-Occurring Disorders. https://www.samhsa.gov/mental-health/serious-mental-illness/co-occurring-disorders
- QuickFacts: Orange County, California. https://www.census.gov/quickfacts/fact/table/orangecountycalifornia
- Co-occurring mental health and substance use disorders: Epidemiology and treatment. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6762143/
- Substance Use and Co-Occurring Mental Disorders – NIMH. https://www.nimh.nih.gov/health/topics/substance-use-and-mental-health
- Treatment for Substance Use Disorder With Co-Occurring Mental Illness. https://pmc.ncbi.nlm.nih.gov/articles/PMC6526999/
- Licensing and Certification Facility Licensing. https://www.dhcs.ca.gov/provgovpart/Pages/Licensing-and-Certification-Facility-Licensing.aspx
- Mental Health Licensing & Certification Branch. https://www.dhcs.ca.gov/provgovpart/Pages/MH-Licensing.aspx
- Licensing and Certification – Complaints. https://www.dhcs.ca.gov/individuals/Pages/Sud-Complaints.aspx
- Monitoring Californians’ Mental Health: Population Surveillance. https://pmc.ncbi.nlm.nih.gov/articles/PMC6557041/
- QuickFacts: Orange County, California. https://www.census.gov/quickfacts/fact/table/orangecountycalifornia/PST045225



