Key Takeaways
- Alcohol use disorder is a medical condition diagnosed when at least two of eleven DSM-5-TR symptoms appear within a 12-month window, not a moral failing or a drink count 3.
- Severity runs on a spectrum: two to three symptoms is mild, four to five moderate, six or more severe, and someone with a steady job can still meet criteria 2, 3.
- Heavy drinking and alcohol use disorder measure different things, so the line is drawn by symptoms like craving, tolerance, withdrawal, and continued use despite harm, not by weekly volume 1, 3.
- Of 27.9 million U.S. adults and adolescents meeting AUD criteria, only 2.5 percent received medication, making integrated care that treats co-occurring anxiety, depression, or PTSD alongside drinking the practical next step 7, 10.
When drinking stops being a choice and becomes a condition
If you’re reading this, you’re already doing something hard. Maybe you’re trying to figure out whether your own drinking has crossed a line. Maybe you’re worried about someone you love and you don’t want to overreact, but you also don’t want to keep pretending nothing is wrong. Either way, you came here looking for a real answer, not a lecture.
Here is the honest version. What is considered alcohol addiction in modern medicine isn’t a personality flaw, a moral failure, or a label reserved for people who’ve lost everything. It’s a medical condition called alcohol use disorder, or AUD, and it shows up on a spectrum from mild to severe based on specific symptoms a clinician can count 1, 4. Some people meeting criteria still have a job, a marriage, and a clean driving record. Some don’t. Both can be living with the same condition.
What makes it a condition rather than a choice is what alcohol does to the brain over time. Repeated heavy use changes the circuits that handle reward, stress, and self-control, which is why cutting back feels so much harder than it sounds and why relapse is common even after long stretches of not drinking 1, 8. That’s not weakness. That’s biology, and biology responds to treatment. The rest of this article walks you through the criteria, the severity levels, what changes when a mental health condition is also in the picture, and what to do next.
What clinicians actually mean by alcohol use disorder
When a clinician asks about your drinking, they’re not running a tally of how many beers you had last Saturday. They’re listening for a pattern. What is considered alcohol addiction in current medical practice is a diagnosis called alcohol use disorder, defined in the DSM-5-TR as a problematic pattern of alcohol use that causes clinically significant distress or impairment, with at least two of eleven specific symptoms showing up inside the same 12-month window 3. That’s the whole framework. No mention of brown bags. No mention of hitting bottom.
The shift to this single diagnosis matters. The older DSM-IV split things into two boxes called alcohol abuse and alcohol dependence, which forced clinicians (and people trying to understand themselves) to decide which category they fit. DSM-5 collapsed those two into one spectrum and let severity be measured by counting symptoms instead 2. MedlinePlus puts it in the plainest words: alcohol use disorder is drinking that causes distress and harm, and it ranges from mild to severe 4.
There’s another piece worth knowing before the criteria themselves. What is considered alcohol addiction isn’t only about behavior. It’s also about what’s happening underneath. Heavy, repeated drinking changes the brain’s reward, stress, and executive-control circuits in ways that drive craving and make stopping genuinely difficult 8. That’s why so many people describe trying to cut back and being surprised by how much harder it is than they expected. Your brain is doing exactly what brains do when those circuits get rewired. It isn’t proof you lack willpower.
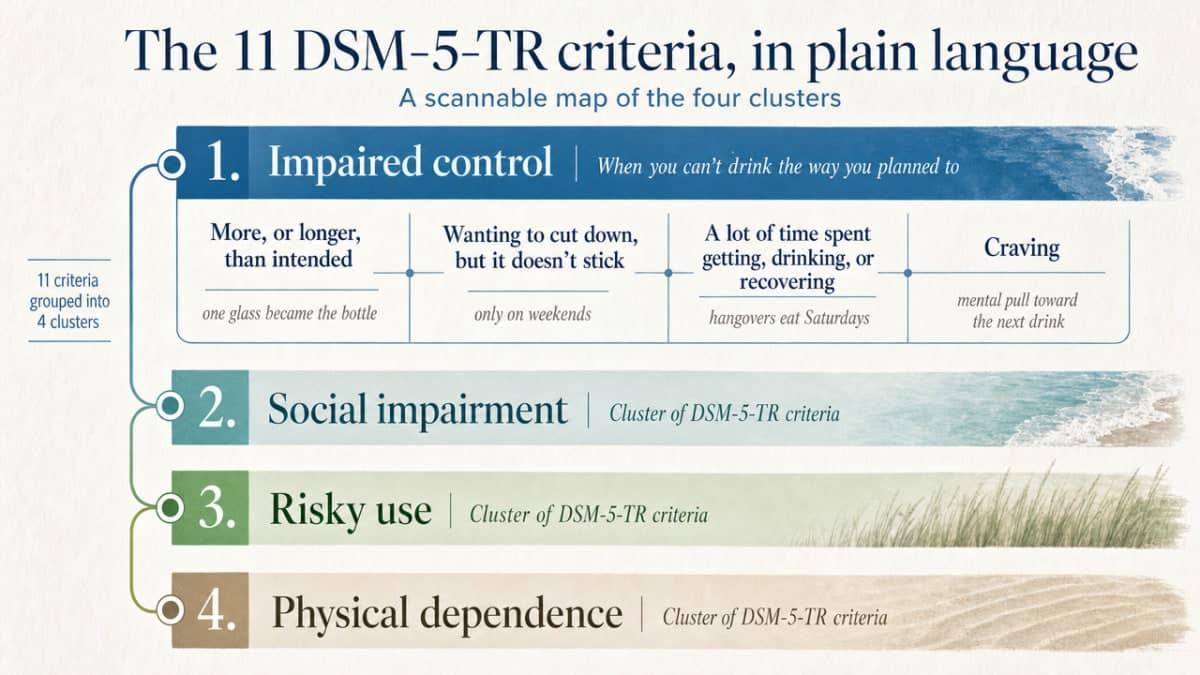
The 11 DSM-5-TR criteria, in plain language
Impaired control: when you can’t drink the way you planned to
The first cluster of criteria is about the gap between what you intended and what actually happened. Four of the eleven DSM-5-TR symptoms live here 3.
The first is drinking more, or for longer, than you meant to. You poured one glass and somehow finished the bottle. You went out for a drink after work and got home at midnight. The second is wanting to cut down or stop, and trying, and not being able to make it stick. Maybe you’ve done Dry January and watched it collapse by January 6th. Maybe you’ve promised yourself “only on weekends” so many times the phrase has lost meaning.
The third is spending a lot of time getting alcohol, drinking it, or recovering from it. Hangovers that eat your Saturdays count. So does mental real estate spent planning around the next drink. The fourth is craving, that pull toward alcohol that shows up without warning and makes it hard to think about much else 8. This is part of what is considered alcohol addiction at the brain level, not a character problem you can argue yourself out of.
Social impairment: when drinking starts costing you people and roles
The next three criteria are about what alcohol is taking from the rest of your life 3.
The first: drinking is getting in the way of what you’re supposed to be doing. Missed mornings at work. Showing up but not really there. Forgetting to pick someone up, or doing it with a headache so bad you can barely talk. The second: you keep drinking even though it’s hurting your relationships. The same fight with your partner, on a loop. A friend who stopped calling. A teenager who’s started watching you a little too carefully.
The third is quieter, and it tends to sneak up on people. You’ve given up things you used to care about, or cut back on them, because drinking took the room. The hike you used to do every Saturday. The band you played in. The Sunday dinners you used to host. None of these alone defines what is considered alcohol addiction, but together they sketch the shape of a life shrinking around alcohol.
Risky use: drinking through warning signs your body and life are giving you
Two of the eleven criteria fall here, and they’re often the ones people dismiss the fastest 3.
The first is using alcohol in situations where it’s physically dangerous. Driving after a few. Mixing it with medications you’ve been told not to mix it with. Drinking around water, around stairs, around anything that needs your full attention. You may have been lucky so far. Luck isn’t the same as safety.
The second is continuing to drink even though you know it’s making a physical or psychological problem worse. Your doctor mentioned your liver enzymes. Your therapist connected your anxiety to your drinking. Your sleep has been a wreck for two years. You heard the information, you may even have agreed with it, and you kept drinking anyway. That isn’t stubbornness. It’s one of the patterns clinicians are trained to recognize as part of what is considered alcohol addiction.
Tolerance and withdrawal: the pharmacological signals
The last two criteria are about what your body has learned to do with alcohol, and they’re some of the clearest signs that drinking has crossed from habit into a medical condition 3.
Tolerance means it takes more alcohol than it used to in order to get the same effect, or that the same amount doesn’t hit the way it once did. You used to feel two drinks. Now four barely register. Withdrawal is the other side: when alcohol leaves your system, your body protests. Shakiness in the morning. Sweating. Nausea. Anxiety that spikes hard around the time you’d usually have a drink. Some people drink in the morning just to make those feelings stop, which is itself a form of withdrawal management.
Together, these four clusters make up the framework:
- Impaired control
- Social impairment
- Risky use
- Tolerance and withdrawal
If two or more of these eleven symptoms have shown up in the same 12-month stretch, that meets the threshold for alcohol use disorder. Two to three symptoms is considered mild, four to five is moderate, and six or more is severe 3. That is what is considered alcohol addiction in current clinical practice, and reading it on a page doesn’t decide anything for you. A real conversation with a clinician does.
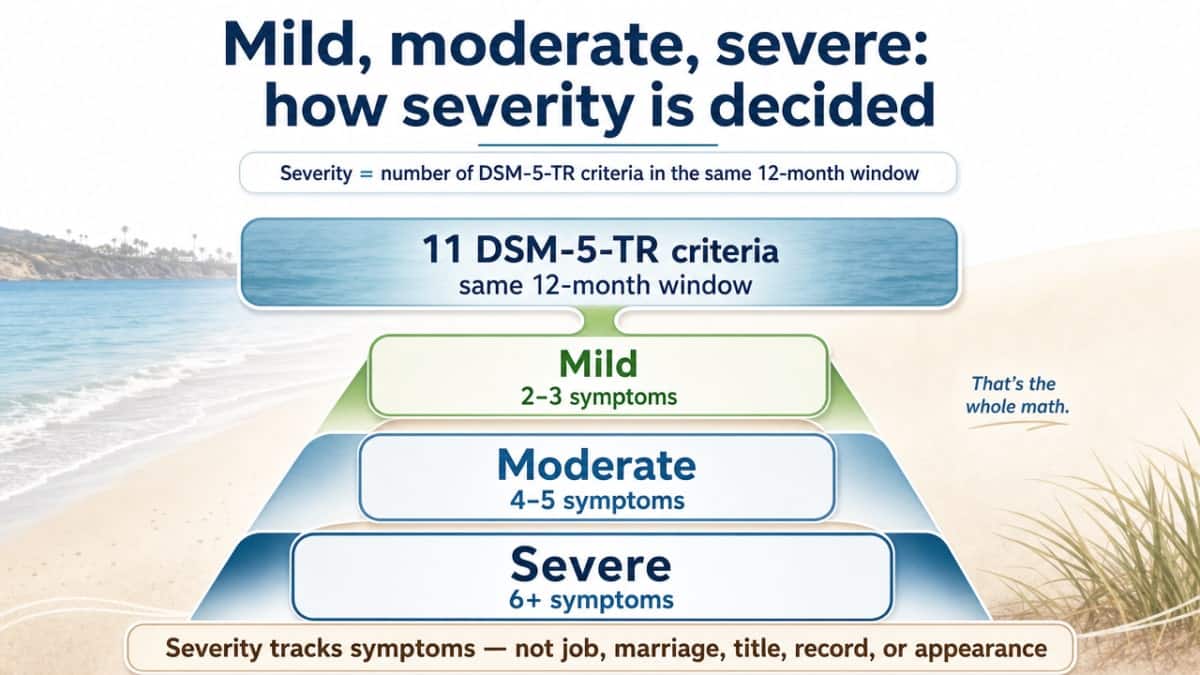
Mild, moderate, severe: how severity is decided
Severity in alcohol use disorder isn’t measured by how dramatic your story sounds. It’s measured by how many of the eleven DSM-5-TR criteria you’ve experienced inside the same 12-month window. Two to three symptoms is mild. Four to five is moderate. Six or more is severe 2, 3. That’s the whole math.
What this means in practice can be hard to sit with. A person who still has a job, a marriage, and a clean record can meet criteria for moderate alcohol use disorder and have no idea, because the picture in their head of what is considered alcohol addiction was built from movies and stereotypes, not from a symptom count. A person whose drinking looks worse from the outside might actually land in the mild range. Severity doesn’t track your zip code or your title at work. It tracks your symptoms.
Heavy drinking vs. alcohol use disorder: the line people keep missing
Heavy drinking and alcohol use disorder are not the same thing, and confusing them is one of the reasons people put off getting help for years. Heavy drinking is a pattern, usually defined by how much and how often. Alcohol use disorder is a diagnosis, defined by what alcohol is doing to your life and your body 1, 3. You can drink heavily for a stretch and not meet criteria. You can also drink less than the heavy-drinking thresholds and still meet criteria if the symptoms are there. The two overlap, but they are not interchangeable.
Here is the part people miss. What is considered alcohol addiction isn’t decided by counting drinks. It’s decided by counting symptoms. A person who has four beers most nights but has never tried to cut back, has no cravings, no withdrawal, no relationship fallout, and no missed responsibilities may be drinking heavily without meeting any DSM-5-TR criteria 3. Another person who drinks twice a week but keeps drinking through warnings from their doctor, has tried and failed to stop, and feels anxious the morning after may already be in the mild range. The volume looks lighter. The condition is real.
If you’re trying to figure out where you land, stop asking whether you drink more than your friends. Ask whether two or more of the eleven criteria have shown up in the last twelve months 3. That’s the line. And it’s a line a clinician can help you draw without judgment.
DSM-5-TR vs. ICD-11: why old binaries no longer hold
You may have grown up with a simple split: people who could handle their drinking, and people who couldn’t. Social drinker on one side, alcoholic on the other. That binary was never very accurate, and the diagnostic systems clinicians use today have moved away from it for good reasons.
The DSM-5-TR, used widely in the United States, treats what is considered alcohol addiction as a single condition called alcohol use disorder, sitting on a continuous spectrum from mild to severe based on how many of eleven symptoms are present in a 12-month window 3, 2. There’s no separate “abuse” box and “dependence” box anymore. The ICD-11, used internationally, still keeps two categories: harmful pattern of use, defined as drinking that has already damaged your physical or mental health or harmed others, and alcohol dependence, marked by impaired control and the brain changes that come with it 5. Researchers have pointed out that this split doesn’t fully capture how alcohol problems actually unfold in real lives, where harm and dependence often overlap 5.
The takeaway is simple. If you’ve been waiting to feel “dependent enough” before taking your drinking seriously, the current science doesn’t support that wait. The spectrum is the point.
Why anxiety, depression, PTSD, and bipolar change how addiction shows up
The overlap: self-medication, shared brain circuits, and missed diagnoses
If you live with anxiety, depression, PTSD, bipolar disorder, or ADHD, what is considered alcohol addiction can look different in your life than it does in a textbook. The drinking often starts as a kind of math. A glass takes the edge off the racing thoughts. Two more help you sleep. A few make the panic that follows a trauma trigger feel survivable for an hour. That isn’t a character flaw. That’s self-medication, and it’s one of the most common reasons people who already carry a mental health condition end up meeting AUD criteria.
The overlap isn’t accidental. Alcohol use disorder is increasingly described as a chronic relapsing brain condition with a strong gene-environment-stress component and significant comorbidity with other mental and physical disorders 9. The same reward, stress, and executive-control circuits that drive craving and loss of control in AUD are circuits that anxiety, depression, and PTSD also pull on hard 8. When two conditions tug at the same wiring, they amplify each other.
This is also why diagnoses get missed. A clinician sees the anxiety and misses the drinking. Another sees the drinking and misses the trauma. The APA’s own guideline notes that AUD frequently appears alongside significant psychiatric comorbidity 10, which is exactly why a single-lens assessment leaves so much out.
Integrated dual diagnosis care, and why one-sided treatment tends to fail
Treating only the drinking, or only the mental health condition, is one of the quietest reasons people cycle in and out of help for years. If you get sober and your untreated PTSD is still firing every night at 2 a.m., the relief alcohol used to provide doesn’t disappear just because the alcohol did. If you start an antidepressant but keep drinking heavily, the medication has a much harder job, and so do you.
Integrated dual diagnosis care treats both at the same time, in the same plan, with clinicians who talk to each other. That usually means a combination of therapy designed for trauma and mood (DBT, CBT, EMDR), psychiatric care with medication management when it’s appropriate, and structured support for the drinking itself, including FDA-approved medications for AUD when indicated 10. The point isn’t to pick which condition is the “real” one. The point is to stop forcing you to choose.
If you’re in Orange County and looking for this kind of care, 449 Recovery in Mission Viejo is one of the local outpatient programs built specifically around co-occurring mental health and alcohol use disorder. What is considered alcohol addiction in your case may not be separable from what else you’re carrying, and good treatment respects that.
Why most people who meet criteria never receive full care
Here is the number that sits behind almost every conversation about what is considered alcohol addiction in this country. SAMHSA’s most recent National Survey on Drug Use and Health found that 27.9 million people in the United States aged 12 or older met criteria for past-year alcohol use disorder, and only 2.5 percent of them, about 697,000 people, received any medication for AUD 7. That’s a population the size of a major state living with a diagnosable condition, and the slice receiving one of the most evidence-based parts of treatment is barely a sliver.
Why the gap? Some of it is stigma. The picture in many people’s heads of what is considered alcohol addiction still looks like a stranger on a park bench, so a person with a steady job and moderate AUD doesn’t recognize themselves in the word and never asks. Some of it is fragmented care. A primary care visit may screen for drinking but rarely connects you to a clinician who can prescribe naltrexone or acamprosate, both of which the APA practice guideline endorses for AUD 10. Some of it is the mental health overlap. If you’re already being treated for anxiety or depression, the drinking can hide in plain sight because no one in the room is asking the right questions 10.
None of that means you’re stuck in that 97.5 percent. It means the system has been quiet about options that exist, and knowing they exist is the first thing that changes for you.

What comprehensive treatment looks like today
Comprehensive treatment for alcohol use disorder in 2025 doesn’t look like the movie version. There’s no single rock-bottom moment, no white-knuckle willpower test, no one-size-fits-all program. What is considered alcohol addiction today is treated the way other chronic conditions are treated: with a combination of approaches matched to your symptoms, your severity level, and whatever else you’re carrying alongside it.
There are usually three legs to that combination. The first is therapy. Cognitive behavioral therapy helps you notice and interrupt the thought-and-feeling loops that lead to a drink. Dialectical behavior therapy builds skills for tolerating the distress that used to send you reaching for one. Trauma-focused work like EMDR addresses the memories that have been quietly driving the drinking in the first place. The second leg is medication. The APA practice guideline endorses naltrexone and acamprosate as first-line pharmacologic options for AUD, both of which reduce craving and support people who are trying to cut back or stop 10. These aren’t sedatives, and they aren’t replacement drinking. They’re tools that work on the same brain circuits the alcohol changed 8.
The third leg is psychiatric care for anything else in the picture. If you also live with anxiety, depression, PTSD, bipolar disorder, or ADHD, your treatment plan needs to address those at the same time, in the same plan, with clinicians who actually talk to each other 10. That integrated approach is what the field means when it says dual diagnosis care, and it’s where outpatient programs like partial hospitalization and intensive outpatient tend to shine, because you can do real clinical work while still living your life. What is considered alcohol addiction in your case is treatable. The shape of that treatment is yours to build with a clinician, not something you have to figure out alone.
If you recognized yourself in the criteria, here is your next step
If two or more of the eleven criteria felt familiar as you read, you don’t have to decide today what to call it or how serious it is. That’s a clinician’s job, and it’s a conversation, not a verdict. What is considered alcohol addiction in your life specifically can only be sorted out by someone who can ask the follow-up questions a page like this can’t.
Here is a reasonable next step. Call an outpatient program that does both mental health and alcohol use disorder under one roof, and ask for an assessment. If you’re in Orange County, 449 Recovery in Mission Viejo offers that kind of integrated dual diagnosis evaluation and outpatient care. Bring what you noticed. Bring the criteria that hit closest. Bring the anxiety or depression or trauma history you’ve been carrying alongside the drinking 10. You don’t need a polished story. You just need to start the conversation. That’s the step. The rest gets built with you, not at you.
Frequently Asked Questions
How many drinks per week is considered alcohol addiction?
There isn’t a drink-count answer, and that’s the honest version. What is considered alcohol addiction is decided by symptoms, not by a number on a weekly tally. The DSM-5-TR asks whether at least two of eleven specific patterns, like craving, loss of control, or continued drinking despite harm, have shown up in the same 12-month window 3. Your drinks-per-week number is information for a clinician, not a verdict.
Can you have alcohol use disorder if you only drink on weekends?
Yes. Frequency isn’t the deciding factor. Someone who drinks only on Friday and Saturday can still meet criteria for alcohol use disorder if they keep drinking despite harm, can’t stop once they start, crave it during the week, or have given up things they used to care about 3. What is considered alcohol addiction is about the symptom pattern across 12 months, not which days the drinking lands on.
What is the difference between heavy drinking and alcohol use disorder?
Heavy drinking describes a pattern of how much and how often. Alcohol use disorder is a medical diagnosis based on whether at least two of eleven DSM-5-TR symptoms are present in a 12-month window 1, 3. You can drink heavily without meeting criteria, and you can drink less than heavy thresholds and still meet them. Volume and diagnosis overlap often, but they’re measuring different things.
If I think I have a drinking problem and also struggle with anxiety or depression, where do I start?
Start with an outpatient program that treats both conditions in the same plan. Alcohol use disorder frequently appears alongside significant psychiatric comorbidity, and treating one side while ignoring the other tends to leave you cycling 10. Ask for an integrated dual diagnosis assessment so therapy, psychiatric care, and AUD treatment get built together. Bring what you’ve noticed about your drinking and your mental health symptoms.
Does meeting two DSM-5-TR criteria really mean I have alcohol use disorder?
Two of the eleven criteria inside a 12-month window meets the threshold for mild alcohol use disorder 2, 3. Mild isn’t a small thing to dismiss, and it isn’t a catastrophe either. It means a clinician would diagnose AUD and that this is often the most responsive point on the spectrum to treat. An assessment confirms whether the symptoms truly cluster the way the criteria describe.
Can alcohol use disorder go away on its own, or is treatment necessary?
Some people reduce or stop drinking without formal treatment, especially in milder ranges. But alcohol use disorder is described as a chronic, often relapsing condition because lasting brain changes drive craving and loss of control well after the last drink 1, 8. Treatment, which can include therapy, FDA-approved medications like naltrexone or acamprosate, and care for co-occurring conditions, gives most people a better shot at lasting change 10.
References
- Understanding Alcohol Drinking Patterns. https://www.niaaa.nih.gov/alcohols-effects-health/alcohol-drinking-patterns
- Alcohol Use Disorder: A Comparison Between DSM–IV and DSM–5. https://www.niaaa.nih.gov/publications/brochures-and-fact-sheets/alcohol-use-disorder-comparison-between-dsm
- Alcohol Use Disorder: From Risk to Diagnosis to Recovery. https://www.niaaa.nih.gov/health-professionals-communities/core-resource-on-alcohol/alcohol-use-disorder-risk-diagnosis-recovery
- Alcohol Use Disorder (AUD) – MedlinePlus. https://medlineplus.gov/alcoholusedisorderaud.html
- ICD‐11 for Alcohol Use Disorders: Not a Convincing Answer to the Challenges of Diagnosing Alcohol Use Disorders. https://pmc.ncbi.nlm.nih.gov/articles/PMC6899584/
- Facts About U.S. Deaths from Excessive Alcohol Use. https://www.cdc.gov/alcohol/facts-stats/index.html
- SAMHSA Releases Annual National Survey on Drug Use and Health. https://www.samhsa.gov/newsroom/press-announcements/20250728/samhsa-releases-annual-national-survey-on-drug-use-and-health
- Alcohol use disorder: pathophysiology, effects, and pharmacologic options. https://pmc.ncbi.nlm.nih.gov/articles/PMC3931699/
- The NIDA Brain Disease Paradigm: History, Resistance and Spinoffs. https://digitalcommons.unf.edu/cgi/viewcontent.cgi?article=1000&context=ahis_facpub
- The American Psychiatric Association Practice Guideline for the Pharmacological Treatment of Patients With Alcohol Use Disorder. https://pubmed.ncbi.nlm.nih.gov/29301420/



