Key Takeaways
- Treatment moves through three phases: stabilization and skills, gradual memory processing, and integration into daily life, with the early weeks designed to feel calmer than expected 1.
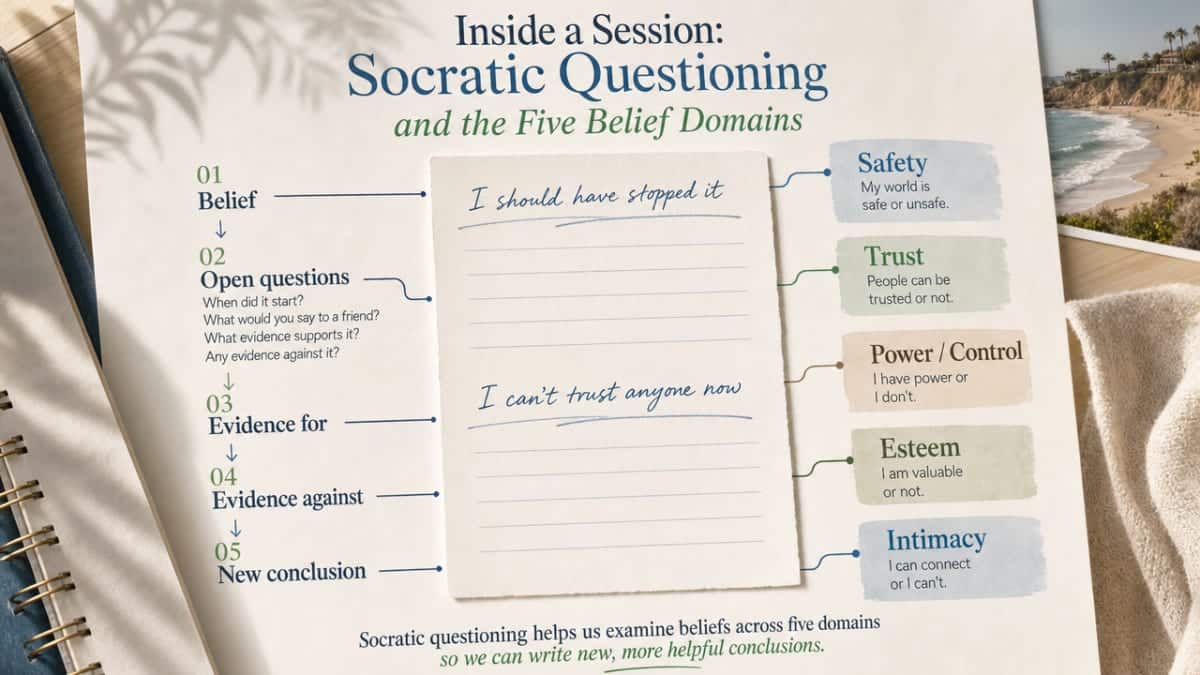
- Socratic questioning sits at the center of session work, examining beliefs across five domains the trauma tends to disrupt — safety, trust, power and control, esteem, and intimacy 4.
- Evidence holds across populations: a Hedges’ g of 1.71 in pediatric outcomes at 12-month follow-up 8, and meaningful symptom reductions in routine adult outpatient care 2.
- Fit, pacing, and co-occurring care matter most when choosing a therapist — ask about training, how they sequence skills before memory work, and how they handle symptom spikes between sessions 9.
What the First Few Weeks Actually Feel Like
You walk into the first session braced for the worst. You expect to be asked, right away, to describe the thing that hurt you. That is almost never how trauma focused cognitive behavioral therapy actually begins.
The early weeks are quieter than you’d guess. Your therapist asks about sleep, about what sets your shoulders tight, about how you’re getting through Tuesdays. You map out what trauma does inside the body — the racing heart, the foggy memory, the way certain smells or sounds can drop you into a different decade. That’s psychoeducation, and it sounds clinical, but in the room it feels more like someone finally explaining why you’ve been reacting the way you have. Nothing is broken in you. Your nervous system learned to protect you, and now it needs new instructions.
You’ll likely learn a few grounding skills before week three — paced breathing, a simple way to notice five things in the room, maybe a worksheet that helps you name what you’re feeling without spiraling into it. These tools are not filler. They’re the safety net your therapist is weaving before any harder work begins 1.
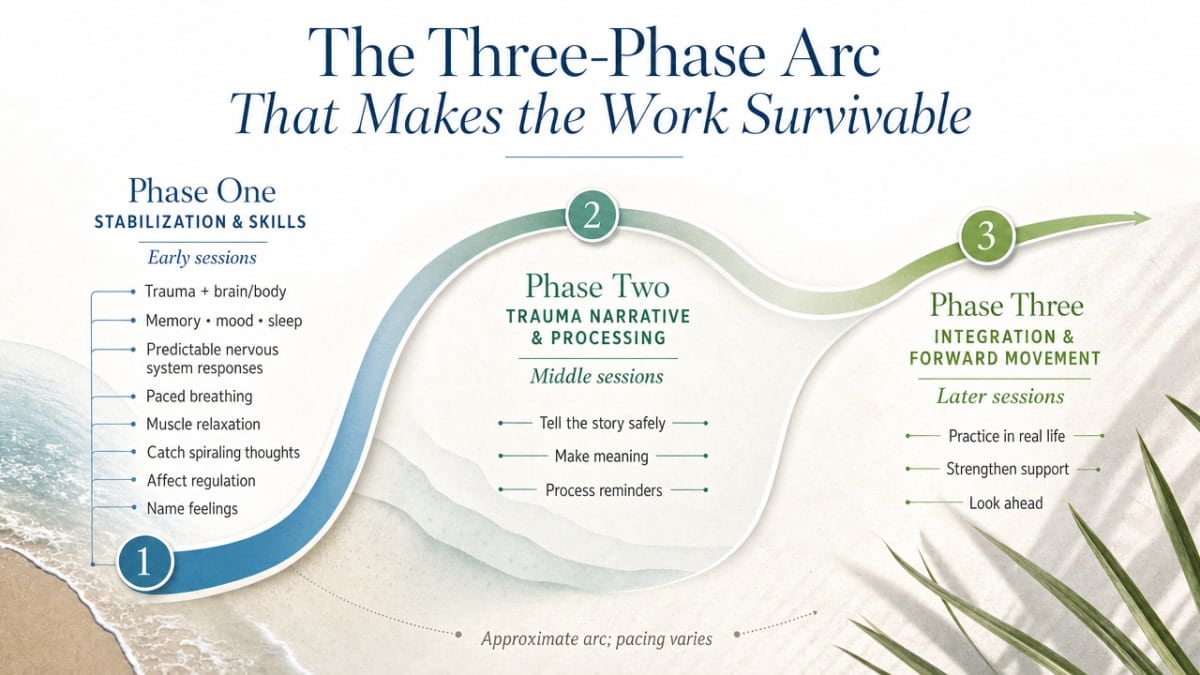
The Three-Phase Arc That Makes the Work Survivable
Phase One: Stabilization and Skills Before Anything Else
The first phase of trauma focused cognitive behavioral therapy is the part most people don’t expect. You’re not diving in. You’re getting steady.
Your therapist spends these early sessions teaching you what trauma does to the brain and body, walking through how memory, mood, and sleep all tangle together after something hard happens. You learn that the racing thoughts and the numb stretches and the way your body sometimes feels like it isn’t yours — those aren’t character flaws. They’re predictable responses your nervous system built to keep you safe 1.
Then come the tools. Paced breathing. Muscle relaxation. A few cognitive strategies for catching the thoughts that send you spiraling at 2 a.m. Affect regulation work — naming what you feel, in finer detail than “bad” or “fine.” Many programs build in a short worksheet routine here, partly because it gives you something tangible to take home, and partly because skill practice between sessions is where most of the real change quietly happens 6.
Phase one usually runs the first third of treatment. In a typical course of trauma focused cognitive behavioral therapy, that means roughly four to six sessions out of the standard 12 to 16 1. Some people need longer here, and a good therapist will give it to you. The point of this phase isn’t to rush past your distress. It’s to make sure that when you do approach the memory in phase two, you’ve got real ground under your feet.
If phase one feels almost boring at moments, take that as a good sign. Boring means your nervous system is settling.
Phase Two: Processing the Memory, Not Reliving It
Phase two is the one people fear before they start, and the one they often describe differently afterward.
This is where trauma focused cognitive behavioral therapy turns toward the memory itself. The work is gradual on purpose. You and your therapist build what’s often called a trauma narrative — a written or spoken account of what happened, developed in small pieces across several sessions. You might start with the least distressing edges of the story and move inward only as your tolerance grows 1. Some protocols use a written account; others, like cognitive processing therapy, can produce strong results without a detailed written narrative, focusing instead on the beliefs the trauma left behind 4.
The key word here is processing, not reliving. Reliving is what your nervous system has been doing on its own — at night, in flashbacks, in the seconds after a trigger. Processing is different. You stay in the present with your therapist while you turn toward the memory. You use the skills from phase one. You notice when your body shifts, and you slow down. You learn that the memory can be visited and left, that you can put it down at the end of the hour.
Cognitive work runs alongside the narrative. Your therapist asks Socratic questions — gentle, open questions designed to help you examine thoughts like It was my fault or I should have known without arguing with you about them 4. The aim isn’t to convince you of anything. It’s to help you see the thought clearly enough to decide whether it’s actually true.
Phase two is harder than phase one. It can also be where people first feel something loosen. Many describe it as the memory becoming smaller — not gone, just no longer the size of the room.
Phase Three: Integration and Bringing It Back to Daily Life
By the time you reach phase three, the worst of the heavy lifting is behind you. This last stretch is about taking what you’ve built and folding it back into your actual life.
You and your therapist review the trauma narrative you developed and notice how differently it lands now. You talk about safety planning — not in a crisis sense, but in a practical one. What situations still feel hard? What triggers are likely to show up at family gatherings, at work, in relationships? You rehearse responses. You practice asking for what you need 1.
This phase is also where the gains start to stick. Skills get used in the wild, not just in session. You might catch yourself naming a feeling before it floods you, or grounding yourself in line at the grocery store without making a production of it. Trauma focused cognitive behavioral therapy is designed to leave you with portable tools, not a dependence on the therapy room 6.
The last few sessions usually slow down. You and your therapist review what’s changed, what you want to keep practicing, and what relapse signals to watch for. Ending well is part of the treatment. You’re not being discharged from your story — you’re walking out with a different relationship to it.
Inside a Session: Socratic Questioning and the Five Belief Domains
Step into a mid-treatment session and the room often looks calmer than you’d expect. You and your therapist are sitting with a worksheet between you. There’s a thought written at the top — something like I should have stopped it or I can’t trust anyone now — and the conversation is moving slowly around it.
This is Socratic questioning in practice. Your therapist isn’t telling you the thought is wrong. They’re asking open, careful questions: When did you first start believing that? What would you say to a friend who told you the same thing? What evidence do you have for it — and is there any evidence against it? The questions are gentle, but they’re doing real work. They’re helping you notice that a belief which felt like fact is actually a conclusion your mind drew under impossible conditions 4.
Cognitive processing therapy, one of the most widely used adult protocols inside trauma focused cognitive behavioral therapy, organizes much of this work around five belief domains the trauma tends to disrupt: safety, trust, power and control, esteem, and intimacy 4. You might find that the event taught your nervous system the world isn’t safe — anywhere. Or that no one can be trusted, including yourself. Or that you have no real power over what happens to you. Or that you’re somehow less than you were. Or that closeness with another person now feels dangerous.
Sessions move through these domains over time. You and your therapist take one belief, examine where it came from, and look at how it shows up in your week. A worksheet might ask you to track the thought, your feelings around it, and what happens in your body when it surfaces. Homework between sessions matters here — not as busywork, but because the brain learns through repetition outside the room 4.
What surprises people most is how unhurried this work feels. Trauma focused cognitive behavioral therapy isn’t about catching you in a distortion. It’s about sitting beside you while you look at a belief that has been running your life and asking, together, whether it still fits.
What the Evidence Actually Shows
You deserve to know what the research really says about trauma focused cognitive behavioral therapy — not the marketing version, the actual version, scope and limits included.
The strongest single data point comes from pediatric work. A systematic review and meta-analysis tracking children and adolescents through trauma focused cognitive behavioral therapy found a large overall effect on post-traumatic stress symptoms from pre-treatment all the way out to 12-month follow-up, with a Hedges’ g of 1.71 8. In plain language: the gains were big, and they held. A year after treatment ended, kids who had completed the work were still better. That’s a level of durability most psychotherapy interventions don’t reach.
You should also know what that number doesn’t mean. It comes from studies of children and teens, often with caregiver involvement built into the protocol 1. It is not a promise that your adult outcome will land at the same effect size. The adult evidence base for trauma focused cognitive behavioral therapy — including cognitive processing therapy and prolonged exposure — is robust in its own right, but the data points look different, and the studies were designed for different populations.
For adults, the more useful evidence comes from two directions. First, the VA/DoD 2023 Clinical Practice Guideline for PTSD recommends individual, manualized trauma-focused psychotherapies, including trauma focused cognitive behavioral therapy variants, as first-line treatments over medication alone — including for adults with co-occurring conditions 9. That’s not a soft endorsement. That’s the clinical standard.
Second, a 2025 study of routine outpatient care found that trauma focused cognitive behavioral therapy still produces meaningful reductions in PTSD symptoms when delivered in everyday community settings, not just research clinics with hand-picked participants 2. That matters for you. It means the model holds up where you’d actually receive it.
The honest summary: the evidence for trauma focused cognitive behavioral therapy is strong, it spans age groups, and it survives the messy real-world conditions of community outpatient care. Outcomes vary from person to person — they always do — but the floor of what you can reasonably expect is higher here than with most alternatives.
Why People Leave Treatment Early — and What Helps Them Stay
Here’s the part of the conversation most trauma focused cognitive behavioral therapy explainers skip: a lot of people don’t finish. A 2025 meta-analysis of trauma-focused CBT for PTSD in naturalistic outpatient settings — meaning real community clinics, not tightly controlled research trials — found a weighted average dropout rate of 41.5% across randomized and non-randomized studies 3. Roughly four in ten people who start the work walk away before they reach the end.
You should know that number going in. Not because it’s a reason to hesitate, but because it tells you something honest about what this treatment asks of people, and what good programs do to meet that ask.
People leave for reasons that make sense:
- Phase two can stir up symptoms before it settles them.
- Life gets in the way — work shifts, childcare gaps, a relapse, a hospitalization.
- Some folks discover their therapist isn’t the right fit and don’t know they’re allowed to say so.
- Others reach a moment of relief in phase one and figure that’s enough, not realizing the deeper change is still ahead.
None of these reasons make someone a failure. They make someone human, trying to do hard work in a complicated life.
What helps people stay looks less dramatic than you’d expect:
- Pacing that respects your nervous system, not a calendar.
- A therapist who checks in about your between-session symptoms and adjusts.
- Realistic expectations set on day one — including the fact that some weeks will feel heavier than others.
- Skills practice strong enough in phase one that you don’t enter phase two empty-handed 1.
- Programs that wrap trauma focused cognitive behavioral therapy inside broader support — psychiatric care if you need it, peer connection, treatment for co-occurring conditions — so the therapy hour isn’t carrying your entire recovery 2.
If you’ve started trauma focused cognitive behavioral therapy before and stopped, that history isn’t a verdict. Many people who complete the work the second or third time around describe the earlier attempts as part of how they got ready. You’re allowed to come back. You’re allowed to ask for a different pace, a different therapist, a different sequence. The goal isn’t to white-knuckle your way through a manual. It’s to finish with something that actually changed.

TF-CBT With Co-Occurring Conditions: Substance Use, Depression, Anxiety
Most people walking into trauma focused cognitive behavioral therapy aren’t dealing with PTSD alone. There’s usually a second story running alongside it — a drinking pattern that started after the assault, a depression that settled in years ago and never fully lifted, an anxiety that makes the grocery store feel like a battlefield, a compulsion that keeps the day organized enough to function. Trauma rarely arrives by itself.
The good news: trauma focused cognitive behavioral therapy was built with this in mind. The original research base shows reductions not only in PTSD symptoms but in depression, anxiety, and behavior problems that travel with trauma 1. And the VA/DoD 2023 guideline specifically names trauma-focused psychotherapies as first-line care for adults with PTSD, including those carrying co-occurring conditions 9. You don’t have to get your other symptoms “clean” before this work can begin.
How it actually plays out depends on what you’re carrying. If substance use is part of the picture, your team will usually want some stability in that area first — not full abstinence as a gate, but enough steadiness that phase two won’t pull you under. Many integrated outpatient programs run trauma focused cognitive behavioral therapy in parallel with substance use treatment, so the trauma work and the recovery work reinforce each other rather than compete. When depression is the loudest voice in the room, the cognitive restructuring inside trauma focused cognitive behavioral therapy tends to lift mood as the trauma loses its grip 2. With anxiety or OCD, the gradual exposure skills you build in phase one often transfer directly — the same nervous system you’re teaching to tolerate a memory can learn to tolerate the urge to check the lock one more time.
What matters most is that your treatment team sees the whole picture, not just the PTSD diagnosis. Ask whether your clinician has experience with co-occurring presentations. Ask how trauma focused cognitive behavioral therapy will be sequenced with the rest of your care. You’re allowed to want one plan, not three.
Adapting the Model for Complex PTSD and Adult Survivors
Most of the foundational research on trauma focused cognitive behavioral therapy was built around children and adolescents recovering from single-event traumas — a car accident, a disaster, a specific assault 1. If you’re an adult who grew up inside something — chronic abuse, neglect, ongoing violence, a household where the threat never really turned off — the textbook version of the model wasn’t originally written with you in mind.
That doesn’t mean it can’t reach you. It means the model has to be adapted, and the good news is that the adaptation has its own evidence base. A meta-analysis of trauma-focused psychotherapy for complex PTSD found that approaches in the trauma focused cognitive behavioral therapy family produce meaningful improvements in CPTSD symptoms, depression, and functional impairment when they’re paced and sequenced for the population they’re treating 10.
What does that look like in practice? Phase one tends to run longer. You may spend more weeks building emotion regulation skills, working on self-concept, and rebuilding a sense that other people can be safe — because for complex trauma survivors, those foundations were never reliably there to begin with. Trust with your therapist is part of the treatment, not a prerequisite for it. Phase two often unfolds in smaller pieces, with the trauma narrative addressed in layers rather than a single arc, because there usually isn’t one event to process. There are patterns, periods, relationships.
The five belief domains from cognitive processing therapy — safety, trust, power and control, esteem, intimacy — tend to all be in play for complex trauma survivors, often deeply 4. Your work may move through each one rather than focus on a single hot spot. That’s not a sign the treatment is failing. It’s a sign your story has more chapters, and trauma focused cognitive behavioral therapy is being shaped to meet them.
Finding a Therapist and Knowing What to Ask
The right therapist makes the work feel possible. The wrong one can make you wonder if you’re the problem, when really it’s the fit. You’re allowed to be choosy here.
Start with training. Trauma focused cognitive behavioral therapy is a specific model with formal certification pathways, and many adult clinicians are trained in related protocols like cognitive processing therapy or prolonged exposure 4. A good first question on a consultation call: What’s your training in trauma focused cognitive behavioral therapy or related trauma-focused protocols, and how often do you use it? You’re not being rude. You’re doing due diligence on the person who’s about to sit with you through hard hours.
Ask how they pace the work. A clinician who answers with some version of “we build skills first, we don’t rush into the memory” is speaking the language of the model 1. Ask what they do when a client’s symptoms spike between sessions, and how they handle co-occurring conditions if that’s part of your picture 9. Ask what ending treatment usually looks like in their practice.
Pay attention to the consultation itself. Did they explain things in language you understood? Did you feel rushed, or met? Trust your read. If the first therapist isn’t right, the next one might be — and starting over isn’t starting from scratch. You’re carrying everything you’ve already learned with you.
Frequently Asked Questions
How long does trauma focused cognitive behavioral therapy usually take?
Most courses of trauma focused cognitive behavioral therapy run about 12 to 16 sessions, usually weekly 1. Adults with complex trauma or co-occurring conditions often need longer, especially in phase one. The timeline isn’t a race. A good therapist paces the work to your nervous system, not the calendar, and adjusts as your symptoms shift.
Will I have to talk about my trauma in detail right away?
No. Trauma focused cognitive behavioral therapy is built to delay that part on purpose. The first several sessions focus on understanding what trauma does to your body and learning grounding and coping skills 1. Only after that foundation is steady does the work turn toward the memory itself, and even then it moves in small, manageable pieces you stay in charge of.
Does trauma focused cognitive behavioral therapy work for adults, or is it mainly for kids?
Both. The pediatric evidence base is the deepest, but adult protocols like cognitive processing therapy and prolonged exposure sit inside the trauma focused cognitive behavioral therapy family and are recommended as first-line PTSD treatment for adults by the VA/DoD 2023 guideline 9. Routine outpatient studies confirm the model holds up for adults in community care, not just research settings 2.
Can I do TF-CBT if I’m also dealing with substance use, depression, or anxiety?
Yes. Trauma focused cognitive behavioral therapy was designed with co-occurring symptoms in mind, and current guidelines recommend it for adults with PTSD alongside other conditions 9. The research shows it reduces depression and anxiety symptoms along with PTSD 1. Substance use is usually addressed in parallel, with enough stability in place that phase two work doesn’t pull you under.
What if I start TF-CBT and feel worse before I feel better?
That happens for some people, especially as phase two begins. It doesn’t mean the treatment is failing — it means hard material is moving. Tell your therapist. A skilled clinician will slow the pace, return to grounding skills, or adjust the sequence. The goal of trauma focused cognitive behavioral therapy is steady processing, not white-knuckling through distress. You’re allowed to ask for adjustments.
How do I know if a therapist is actually trained in trauma focused cognitive behavioral therapy?
Ask directly. Trauma focused cognitive behavioral therapy has formal certification pathways, and related adult protocols like cognitive processing therapy have their own training tracks 4. Ask how often they use the model, how they pace phase one, and how they handle symptom spikes between sessions. A clinician trained in this work will describe a clear arc — skills first, then processing, then integration 1.
References
- Trauma-Focused Cognitive Behavioral Therapy. https://pmc.ncbi.nlm.nih.gov/articles/PMC4396183/
- Effectiveness in routine care: trauma-focused treatment for PTSD. https://pmc.ncbi.nlm.nih.gov/articles/PMC11827035/
- Dropout From Trauma-Focused Treatment for PTSD in a Naturalistic Outpatient Setting: A Meta-Analysis and Meta-Regression Analysis. https://pmc.ncbi.nlm.nih.gov/articles/PMC11960572/
- Cognitive Processing Therapy for PTSD. https://www.ptsd.va.gov/professional/treat/txessentials/cpt_for_ptsd_pro.asp
- Effectiveness of Trauma-Focused Cognitive Behavioral Therapy in Treating Children With Post-Traumatic Stress Disorder. https://clinicaltrials.gov/study/NCT00614068
- Trauma-Focused Cognitive Behavioral Therapy (TF-CBT) – SAMHSA. https://www.samhsa.gov/resource/dbhis/trauma-focused-cognitive-behavioral-therapy-tf-cbt
- Trauma Focused CBT – Title IV-E Prevention Services Clearinghouse. https://preventionservices.acf.hhs.gov/programs/904/show
- Stability of Treatment Effects and Caregiver-Reported Outcomes. https://pmc.ncbi.nlm.nih.gov/articles/PMC10981190/
- VA/DoD 2023 Clinical Practice Guideline for the Management of PTSD. https://www.ptsd.va.gov/professional/treat/txessentials/cpg_ptsd_management.asp
- The effectiveness of trauma-focused psychotherapy for complex post-traumatic stress disorder: A meta-analysis. https://pmc.ncbi.nlm.nih.gov/articles/PMC9879871/



