Key Takeaways
- A partial hospitalization program in Mission Viejo bridges the gap between inpatient discharge and weekly outpatient therapy, offering roughly 20–30 hours of weekly structure while you sleep at home.
- Mission Viejo’s suburban commuter setting makes daily attendance feasible, but drive time on the 5 and 73, parking, and backup transportation should weigh into program choice alongside clinical fit.
- Strong programs treat co-occurring mental health and substance use as the default through integrated care, and hold verifiable DHCS licensing, CARF accreditation, and credentialed clinicians 2, 9.
- Before starting, compare daily schedule structure, team communication, after-hours crisis protocols, and a concrete step-down plan into IOP and aftercare so the handoff is built in from day one 1.
The week after discharge is the hardest part
You probably already know this, but it’s worth saying out loud: leaving inpatient care can feel almost as scary as going in. For days or weeks, someone watched your medications, planned your meals, and kept the schedule moving. Then the door opens, the discharge paperwork is signed, and suddenly you’re standing in your kitchen wondering what to do at 10 a.m. on a Tuesday.
That gap is where a lot of recoveries wobble. The structure is gone. The triggers you stepped away from are still in your phone, your neighborhood, and sometimes your own living room. You’re trying to remember the coping skills you just learned while also figuring out what’s for dinner. It’s a lot to hold at once, and feeling overwhelmed doesn’t mean you’re failing. It means the transition is real.
This is exactly the moment a partial hospitalization program Mission Viejo is built for. PHP is the step-down level designed to keep clinical intensity high while you sleep at home and slowly reconnect with daily life 4. You get the structure of treatment most of the day, then practice what you learned in your actual environment by night. For many people stepping out of inpatient psychiatric or substance use care, that bridge is what makes the new skills stick 11.
If you’re reading this for yourself or for someone you love, take a breath. You’re already doing the hard part by looking for the next right step.
Where PHP sits between inpatient and IOP
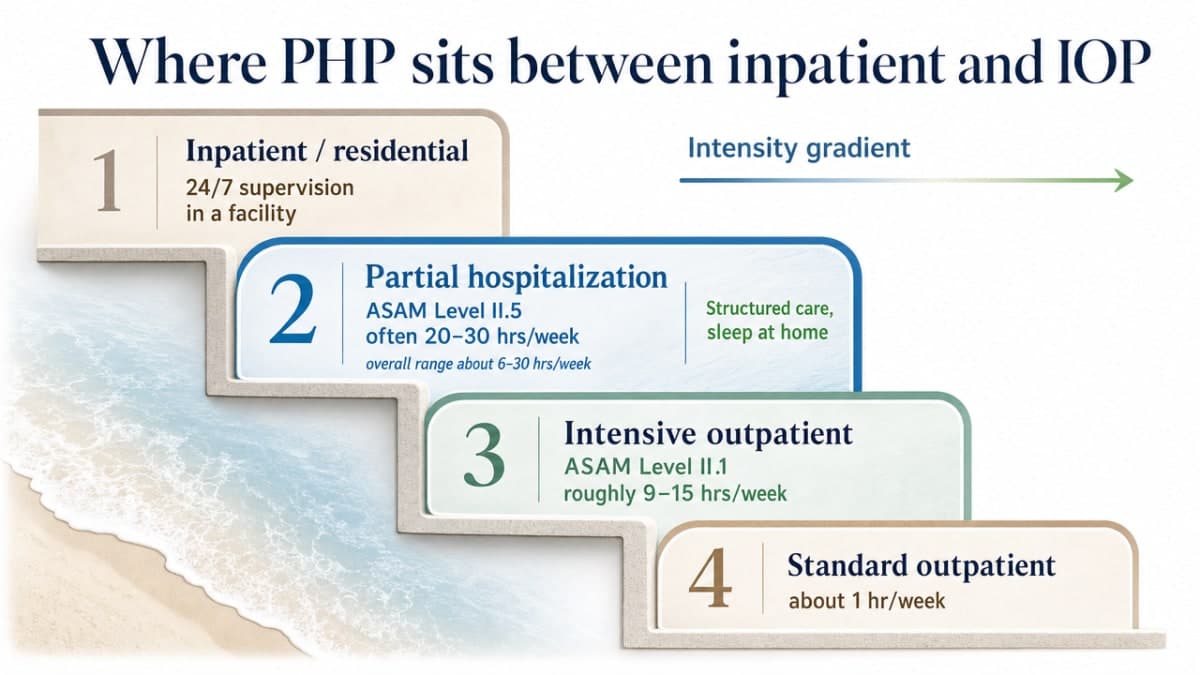
Think of mental health and addiction care as a staircase, not a switch. At the top, inpatient hospitalization wraps around you 24 hours a day. At the bottom, standard outpatient therapy might mean a single one-hour session each week. A partial hospitalization program Mission Viejo lives in the upper-middle of that staircase, close enough to inpatient that the structure still feels real, but far enough down that you sleep in your own bed 4.
Here is the rough shape of the intensity gradient, drawn from ASAM’s continuum-of-care framework 6:
- Inpatient/residential: 24/7 supervision in a facility
- Partial hospitalization (ASAM Level II.5): often 20–30 hours per week, within an overall range of about 6–30 hours
- Intensive outpatient (ASAM Level II.1): roughly 9–15 hours per week
- Standard outpatient: about 1 hour per week
That spread matters more than it might look on paper. Going from 24-hour care straight to a weekly therapy hour is a cliff. PHP turns the cliff into stairs. You attend treatment most of the day, usually five days a week, then go home in the evening to apply what you practiced. A partial hospitalization program Mission Viejo gives you enough clinical contact to catch a wobble early, while still letting you sit at your own dinner table and sleep next to the people who love you.
IOP comes next on the staircase. It typically meets three days a week for three hours, which is enough to keep momentum but not enough to anchor someone who just left inpatient care 5. That is why most thoughtful step-down plans treat PHP as the first stop after discharge, then transition to IOP once you have steadier ground under your feet 11.
If the difference between PHP and IOP still feels blurry, that is okay. A good intake conversation will sort it out based on your symptoms, your support system, and how you are sleeping, eating, and coping in the first days after discharge. The level of care should match where you actually are, not where you think you should be.
What a PHP day actually looks like in Mission Viejo
One of the most common questions families ask after discharge is simple: what will my day actually feel like? It helps to walk through it, because “20 to 30 hours a week” is an abstraction until you picture yourself living it.
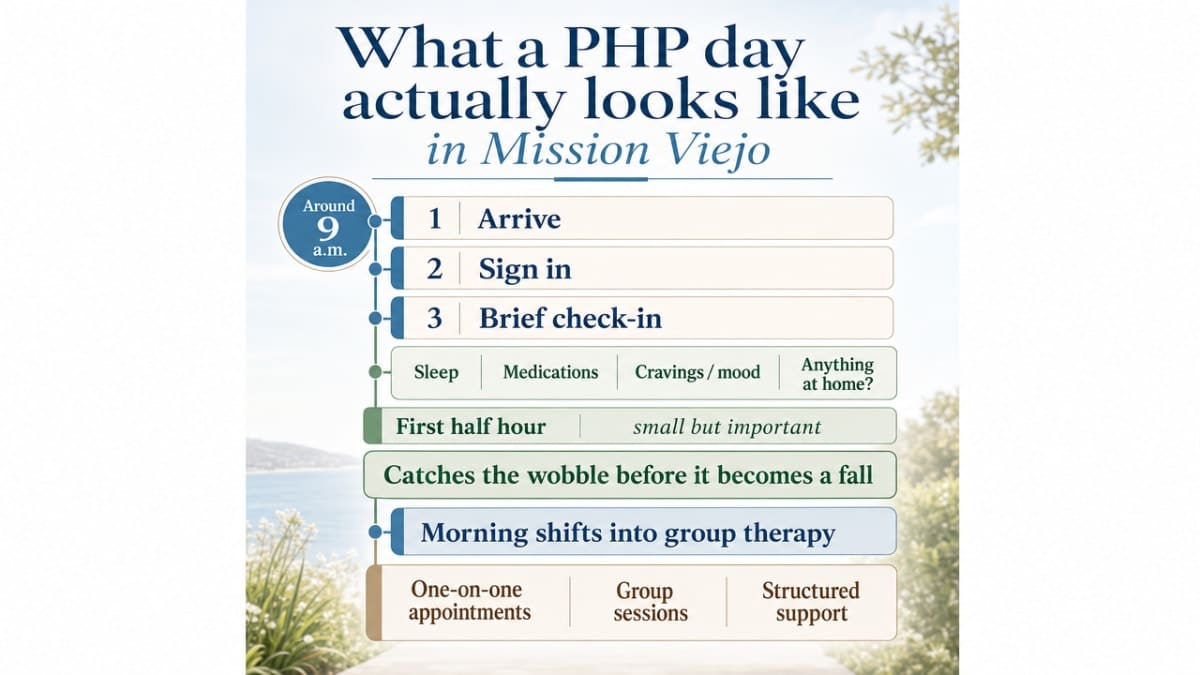
A typical day in a partial hospitalization program Mission Viejo starts mid-morning, usually around 9 a.m. You arrive, sign in, and sit down for a brief check-in. Staff want to know how you slept, whether you took your medications, what your cravings or mood felt like overnight, and whether anything happened at home that needs attention before group starts. This first half hour is small but important. It catches the wobble before it becomes a fall.
From there, the morning shifts into group therapy. A partial hospitalization program Mission Viejo typically includes one-on-one appointments, group sessions, and structured coping-skills education as core elements of the day 5. Groups might focus on relapse prevention, dialectical behavior therapy skills, processing what came up in inpatient care, or working through trauma at a pace that feels manageable. You are not expected to share everything. You are expected to show up.
Lunch is built into the schedule, and it matters more than it sounds. Eating with other people in recovery, even quietly, is part of relearning ordinary rhythms.
Afternoons usually bring an individual therapy session with your assigned clinician, plus skills training and sometimes a psychiatric medication check-in. Family sessions are scheduled weekly or biweekly, because the people you go home to are part of the recovery, not bystanders to it 9. By late afternoon, around 3 or 4 p.m., you are heading home with a small assignment, a coping plan for the evening, and the phone number of someone you can call if things get hard.
That evening piece is where a partial hospitalization program Mission Viejo earns its keep. The work of recovery doesn’t only happen in the group room. It happens when you make dinner without a drink, when you sit with a difficult conversation instead of leaving the house, when you sleep in your own bed and wake up still committed. The structure is intentionally porous so you can practice in the environment you actually live in 11.
Most people attend five days a week to start, then taper as readiness grows. The federal framing of PHP success is exactly this kind of taper, moving someone from 20 hours toward 10, or stepping down to IOP, rather than holding intensity static 1. Your day is not a permanent schedule. It is a temporary scaffold while you rebuild.
Dual diagnosis as the default, not the exception
If you just left inpatient care, there is a good chance you were treated for more than one thing at once. Maybe alcohol use was the headline reason, but anxiety and trauma were running underneath it. Maybe a bipolar diagnosis brought you in, but stimulant use kept making the cycles worse. This pattern is so common that any partial hospitalization program Mission Viejo worth your time should treat dual diagnosis as the starting assumption, not a specialty add-on.
The clinical word for this is co-occurring disorders, and the federal guidance on it is direct: when mental health and substance use show up together, splitting them into two separate treatment tracks usually makes both worse. SAMHSA’s framework calls for integrated care, where the same team addresses both conditions in a coordinated way. The documented benefits include reduced or discontinued substance use, improvement in psychiatric symptoms and functioning, and fewer hospitalizations down the road 9. That last piece matters a lot when you just left a hospital.
What integrated care looks like inside a partial hospitalization program Mission Viejo is less mysterious than it sounds. Your therapist talks to your psychiatrist. Your group leader knows you are tapering off a benzodiazepine and adjusts what they ask of you that morning. The trauma work in individual sessions is paced around your sobriety, not pushed against it. When a craving spikes, the response includes both the mood symptom underneath and the substance behavior on top, in the same conversation.
This sounds obvious, and it often is not the reality on the ground. Some programs still send people to an addiction track in one building and a mental health track in another, with neither team fully in the loop. When you call to ask about a partial hospitalization program Mission Viejo, listen for how they answer questions about both sides of the picture. If the intake coordinator can describe how the psychiatrist, the primary therapist, and the group facilitators share information about you in the same week, that is integrated care. If you hear “we focus on the addiction first and then refer you out for the mental health piece,” that is a referral chain, not a treatment plan.
You are allowed to want a program that holds the whole picture. In fact, holding the whole picture is often what makes the difference between another discharge and a recovery that lasts.
What the evidence actually says about outcomes
You deserve honesty about what a partial hospitalization program Mission Viejo can and cannot do. The research is encouraging, and it also has real limits. Both things are true at once.
Here is what the evidence supports. Studies of adults in acute psychiatric partial hospitalization show that most participants experience meaningful reductions in symptom severity over the course of treatment, with only a small percentage needing rapid rehospitalization 10. When researchers have compared outcomes between PHP and inpatient care for psychiatric patients, they have generally found similar symptom-reduction trajectories across many diagnostic groups, with some evidence of better social functioning among people in day programs 12. Decades of clinical literature describe partial hospitalization as a way to reduce inpatient utilization while maintaining clinical outcomes when it is integrated into a real continuum of care 11.
For families with younger members, a 2024 systematic review of transdiagnostic adolescent PHPs found that every study examined showed improvements in functioning and mental health from admission to discharge 7. That is a consistent signal across different programs and populations.
Now the honest caveats. The adolescent review also noted that only one study included follow-up data after discharge, and only one directly compared PHP to other levels of care 7. Adult comparison studies face their own challenge: people are not randomly assigned to PHP versus inpatient, so selection effects shape who ends up where and what their outcomes look like 12. Single-site adult studies raise generalizability questions about how well any one program’s results predict another 10.
What this means for you is practical. A partial hospitalization program Mission Viejo has a strong evidence base for short-term symptom improvement and a reasonable case for being a clinically sound alternative to extended inpatient stays for many people. What it cannot promise is a guaranteed outcome twelve months from now, because the research itself does not promise that. Anyone telling you otherwise is overselling. The right question is not whether PHP works in general. It is whether this program, for this person, with this support system, sets you up to keep moving forward.
Clinical questions to ask an intake coordinator
When you call a partial hospitalization program Mission Viejo for the first time, you do not need to sound polished or know the right terminology. You are allowed to be tired, scared, or unsure what to ask. Here are the questions that will tell you the most about clinical fit, in language that works on a real phone call.
“How will the program treat both my mental health and any substance use at the same time?” Listen for a clear description of integrated care, not a referral to a separate provider. You want to hear that the same team coordinates psychiatric medication, therapy, and group work for both conditions in the same week 9.
“What does a typical day look like, and how many days a week will I attend?” A solid answer includes specific structural elements like one-on-one sessions, group therapy, and coping-skills education, plus a sense of how the schedule tapers as you progress 5. If the coordinator cannot describe the day, that is information too.
“How does the clinical team share information about me?” The therapist, psychiatrist, and group facilitators should be talking to each other, not just charting in parallel. Ask how often the team meets about your case.
“What is your plan for stepping me down to IOP or aftercare?” A thoughtful program is already thinking about the handoff before you start. Federal guidance frames PHP success as reducing treatment hours or preventing inpatient readmission over time, not holding you at high intensity indefinitely 1.
“What happens if I have a hard night or a craving spikes after hours?” You want to know there is a real protocol, a number to call, and a person who will pick up.
You are not being difficult by asking these questions. You are doing the work of choosing well.
Licensing, credentials, and the California regulatory floor
Here’s something that doesn’t get said enough: not every program calling itself a partial hospitalization program Mission Viejo is operating at the same regulatory standard. California has a real licensing floor, and knowing what to look for protects you from programs that are essentially marketing names without the clinical infrastructure to back them up.
The agency that matters here is the California Department of Health Care Services, specifically its Mental Health Licensing and Certification Branch. This branch provides oversight and determines compliance with state law, regulations, and other governing requirements for mental health treatment programs in California 2. A properly credentialed partial hospitalization program Mission Viejo will be able to tell you, plainly, which state licenses and certifications it holds and which body audits its clinical practices.
Two more credentials are worth asking about directly. The first is CARF accreditation, a voluntary national standard that signals a program has been independently reviewed against quality benchmarks in clinical care, documentation, and client rights. The second is the credentialing of individual clinicians: licensed marriage and family therapists, licensed clinical social workers, licensed psychologists, and board-certified psychiatrists. You are allowed to ask who will be in the room with you, what their license is, and how long they have been doing this work.
Why Mission Viejo geography matters for daily attendance
Here is a practical thing nobody mentions when they hand you the discharge papers: a partial hospitalization program Mission Viejo only works if you can actually get there, five mornings a week, for several weeks in a row. The clinical fit could be perfect on paper, but if the drive falls apart by week two, the treatment falls apart with it.
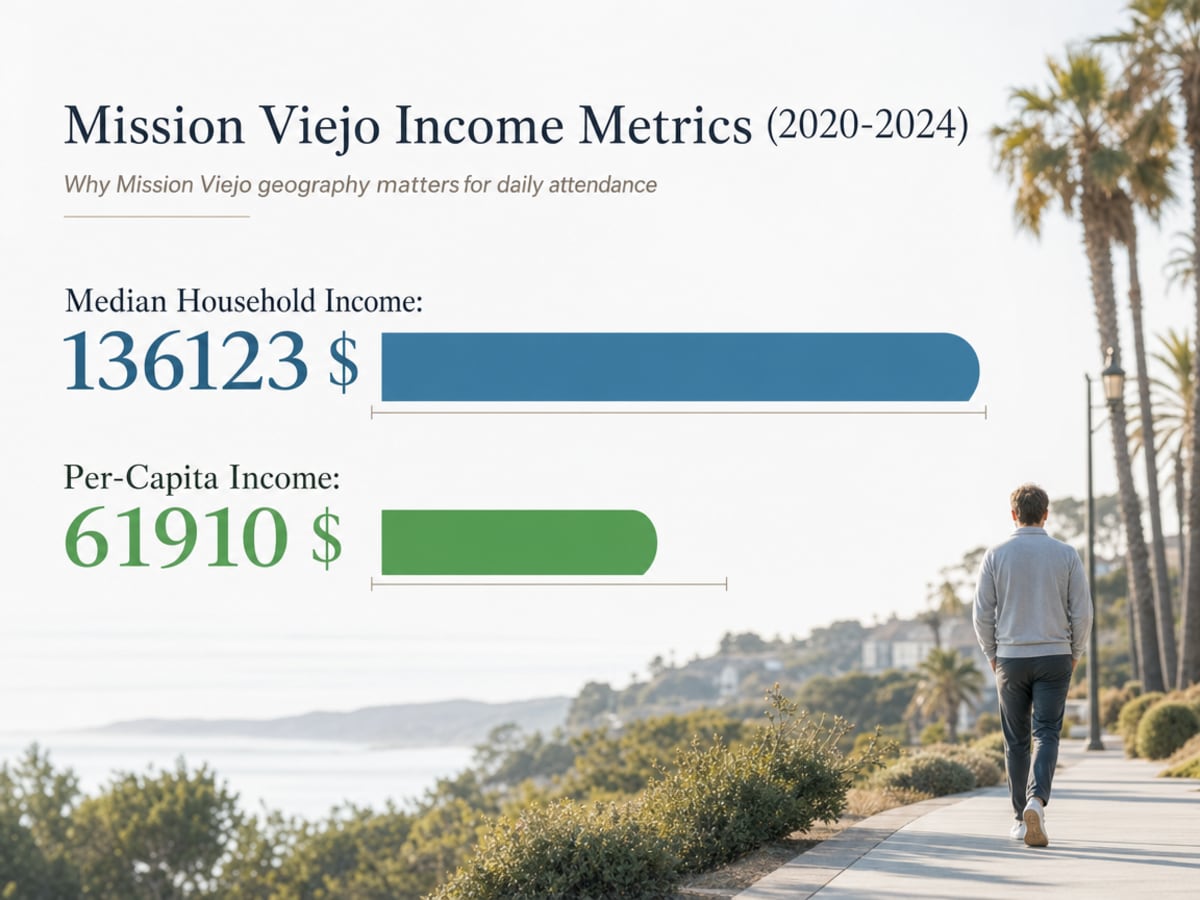
Mission Viejo sits in south Orange County with a population of roughly 93,000 and a median household income of about $136,123, which means you are dealing with a suburban commuter community where most adults are used to driving to work and many have a partner or family member who could share the carpool 3. That matters in both directions. On one hand, the infrastructure for a daily 9-to-3 schedule already exists in most households here. On the other hand, the same traffic patterns on the 5 and the 73 that make a job commute long can make a treatment commute feel impossible after a hard morning group.
When you are choosing a partial hospitalization program Mission Viejo, ask yourself a few honest logistics questions before the clinical ones. How far is the program from your front door in real morning traffic, not Google’s optimistic estimate? Who is your backup driver on the days you do not feel safe behind the wheel? Is there parking, or will hunting for a spot become its own stressor by week three? If you have school-age kids, does the schedule end early enough to handle pickup, or do you need a standing arrangement with another parent?
The reason this matters so much in the first weeks after discharge is that early recovery is fragile in ordinary ways. A 45-minute drive that would be nothing six months from now can feel like climbing a mountain on day four. Picking a program that is genuinely close to home, on roads you already know, removes one of the most common reasons people drop out of step-down care before it has time to work.
Planning the handoff to IOP and aftercare before you start
Here is something most people don’t think about until they’re already in week three: the day you finish a partial hospitalization program Mission Viejo is not the day recovery ends. It is the day the next phase begins. The programs that work best are the ones that started planning that handoff before you even walked in the door.
Ask, during your very first intake call, what the step-down plan looks like. A thoughtful partial hospitalization program Mission Viejo will already have answers. How many weeks does the typical client spend at PHP intensity before transitioning to IOP? Does the same primary therapist follow you down to the next level, or do you start over with someone new? Is there an evening IOP option so you can return to work or school while still getting clinical support? What does aftercare look like at six weeks, three months, and six months out?
The reason this matters is built into how PHP is supposed to function. Federal framing of PHP success centers on moving someone from higher treatment hours toward fewer, or keeping them out of inpatient settings, not holding intensity steady 1. The handoff is the program, in a real sense. Without it, you are just doing weeks of intensive treatment and then falling off a different cliff.
A solid aftercare arrangement usually includes:
- a step into IOP
- continued individual therapy
- psychiatric medication management
- family support
- ongoing connection to community recovery resources or alumni groups
Continuity across that continuum is what the clinical literature describes as the difference between a treatment episode and a sustained recovery 11. You want to leave PHP with names, phone numbers, and a schedule already on the calendar, not a stack of referrals to figure out on your own.
One last encouragement before you make the call. Choosing a partial hospitalization program Mission Viejo is not a test you can fail. It is a decision you can refine. Ask the questions, trust your read of the answers, and remember that the right program will treat your handoff plan with the same care it treats your first day. If you want a place that holds the whole arc with you, 449 Recovery in Mission Viejo is one option worth a conversation.
Frequently Asked Questions
How is a partial hospitalization program Mission Viejo different from an intensive outpatient program?
The main difference is intensity. A partial hospitalization program Mission Viejo usually runs around 20 to 30 hours a week, often five days a week, while IOP typically meets about 9 to 15 hours a week across three or four sessions 6. PHP is the level most people step into right after inpatient care. IOP is where you move next, once your days feel steadier and you are ready to take back more of your regular schedule.
How many hours per week will I spend in a partial hospitalization program Mission Viejo?
ASAM places partial hospitalization in a range of roughly 6 to 30 hours of programming per week, with most adult PHPs landing in the 20-to-30-hour zone during the first weeks of treatment 6. Federal guidance describes PHP as designed to taper over time, often moving someone from 20 hours toward 10 hours as they stabilize, rather than holding intensity static 1. Your specific schedule depends on clinical need and how you are doing week to week.
Can a partial hospitalization program Mission Viejo treat both addiction and mental health conditions at the same time?
Yes, and ideally it should. SAMHSA describes integrated treatment for co-occurring mental health and substance use disorders as the standard, with documented benefits including reduced substance use, improvement in psychiatric symptoms and functioning, and fewer hospitalizations 9. A strong partial hospitalization program Mission Viejo coordinates psychiatric care, individual therapy, and group work for both conditions within the same team. If a program treats addiction and mental health as separate tracks, that is a referral chain, not integrated care.
Do I sleep at home during a partial hospitalization program, or is it residential?
You sleep at home. That is the defining feature of partial hospitalization. You attend structured treatment during the day, usually from mid-morning to late afternoon, then return to your own bed at night 5. This setup is intentional. It keeps clinical intensity high while letting you practice new coping skills in your actual environment, which is part of what makes a partial hospitalization program Mission Viejo such a useful bridge between inpatient care and standard outpatient therapy 11.
How do I know a partial hospitalization program Mission Viejo is properly licensed in California?
California programs offering PHP-level mental health services fall under oversight from the Department of Health Care Services, specifically the Mental Health Licensing and Certification Branch, which determines compliance with state law and regulations 2. Ask any partial hospitalization program Mission Viejo directly which DHCS licenses it holds, whether it is CARF-accredited, and what credentials your primary therapist and medical director hold. A confident, specific answer is a good sign. Vague reassurance is a reason to keep looking.
What happens after I finish a partial hospitalization program?
Most people step down to an intensive outpatient program next, then continue with individual therapy, psychiatric medication management, and some form of community or alumni support. Federal framing describes PHP success as moving you toward fewer treatment hours over time or keeping you out of inpatient settings entirely 1. Clinical literature emphasizes that continuity across these levels is what turns a treatment episode into a sustained recovery 11. The handoff plan should be on the calendar before your last PHP day.
References
- A Study of Partial Hospitalization Programs (PHP) Under the Medicare Partial Hospitalization Program Prospective Payment System. https://www.cms.gov/research-statistics-data-and-systems/statistics-trends-and-reports/reports/downloads/Leung_PHP_PPS_2010.pdf
- Mental Health Licensing & Certification Branch. https://www.dhcs.ca.gov/providers-partners/mental-health-licensing-certification-branch/
- Mission Viejo city, California – QuickFacts. https://www.census.gov/quickfacts/fact/table/missionviejocitycalifornia/PST045224
- The Continuum of Care for Serious Mental Illness. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5394934/
- Treatment Types for Mental Health, Drugs and Alcohol. https://www.samhsa.gov/find-support/learn-about-treatment/types-of-treatment
- Chapter 3. Intensive Outpatient Treatment and the Continuum of Care. https://www.ncbi.nlm.nih.gov/books/NBK64088/
- Review: Patient Outcomes in Transdiagnostic Adolescent Partial Hospitalization Programs. https://pubmed.ncbi.nlm.nih.gov/37271333/
- Monitoring Californians’ Mental Health. https://pmc.ncbi.nlm.nih.gov/articles/PMC6557041/
- Managing Life with Co-Occurring Disorders. https://www.samhsa.gov/mental-health/serious-mental-illness/co-occurring-disorders
- Predictors of outcome of acute partial hospitalization. https://pubmed.ncbi.nlm.nih.gov/10457455/
- Partial hospitalization: A valuable component of the continuum of care. https://pubmed.ncbi.nlm.nih.gov/11527010/
- Outcomes for psychiatric patients in partial hospitalization and inpatient settings. https://pubmed.ncbi.nlm.nih.gov/23280457/



