Key Takeaways
- Evening IOP in Orange County runs roughly three nights a week from 6 to 9 p.m., letting working adults keep their jobs while getting clinical-grade treatment for anxiety, depression, trauma, or substance use.
- Choosing between traditional outpatient, IOP, and PHP should come down to how much structure your symptoms need and how many hours your week can hold, not which program sounds most thorough.
- When mental health and substance use overlap, integrated outpatient care from one team tends to outperform splitting treatment across separate providers and treatment plans 6.
- Before committing, ask whether a program is in-network, offers evening IOP, treats dual diagnosis in-house, and how soon you can start, since parity rules and California network standards often make access faster than expected 13.
What a Tuesday at 6 p.m. Actually Looks Like
It’s Tuesday. You wrapped a status meeting at 4:45, answered three Slack messages in the parking lot, and now you’re driving to a small office in Mission Viejo or Irvine or Tustin. You’re tired. You almost canceled. You didn’t.
At 6 p.m., you sit in a circle of seven other adults who also came straight from work. Someone is still wearing a hospital badge. Someone else has a laptop bag at their feet. A licensed therapist opens the group with a check-in: one word for how you’re walking in. You say “depleted.” Two people nod. Nobody flinches.
The next ninety minutes are not what you pictured. There is no couch, no clipboard quiz, no one asking how your mother made you feel in 1994. Instead, the group works through a specific skill, maybe distress tolerance, maybe a cognitive reframe for the spiral you’ve been having about your inbox. You practice it. You hear how someone else used it on Sunday when their teenager slammed a door. You leave with something you can actually try on Wednesday morning.
This is what flexible outpatient mental health Orange County care looks like for working adults. It is not a 30-day disappearance. It is not a hospital. It is a structured, evidence-based program that meets you after work, takes your job seriously, and treats anxiety, depression, trauma, and co-occurring substance use like the real clinical conditions they are. You go home afterward. You sleep in your own bed. You show up Wednesday. And slowly, something starts to shift.
Why Outpatient Became the Default for Working Adults
For a long time, the unspoken message about serious mental health care was that you had to leave your life to get it. Pack a bag. Tell HR something vague. Hope your manager didn’t ask follow-up questions. That model still exists, and for some situations it’s the right call. But for most working adults dealing with anxiety, depression, trauma symptoms, or a co-occurring substance use issue, it’s no longer the clinically preferred starting point.
The shift is grounded in evidence, not convenience. A 2023 systematic review of integrated versus non-integrated treatment for co-occurring substance use and mental health disorders found that integrated outpatient models often produce better or comparable outcomes in symptom reduction and substance use compared with fragmented, sequential care 14. This means that when the same team treats your depression and your drinking in the same building during the same week, you tend to do at least as well as someone who checks into a residential facility and then tries to find aftercare on the other side. The review looked at adults with dual diagnosis across a range of settings, and while the authors note variability between studies, the directional finding holds.
That matters for you because it means staying employed and staying in treatment are not competing goals. They can reinforce each other. Work gives you structure, identity, and a reason to practice the skills you learn in group on Tuesday night. Treatment gives you the tools to handle the parts of work, parenting, and life that have been quietly grinding you down.
There’s a second reason outpatient has become the working adult’s default: the alternative often delays care. Residential placement requires time off, family logistics, and sometimes a wait. People who can’t make that work frequently do nothing instead. Flexible outpatient mental health Orange County programs lower that barrier. You can start within a week or two, keep your paycheck, and not explain anything to anyone you don’t want to tell.
None of this means outpatient is the right level for every situation. If you’re in acute crisis, having active suicidal thoughts with a plan, or going through a complicated medical detox, you need a higher level of care first. A good intake assessment will tell you that honestly. But for the much larger group of working adults who are functioning on the outside and falling apart on the inside, outpatient is usually where care should begin, not where it ends up after something worse happens.
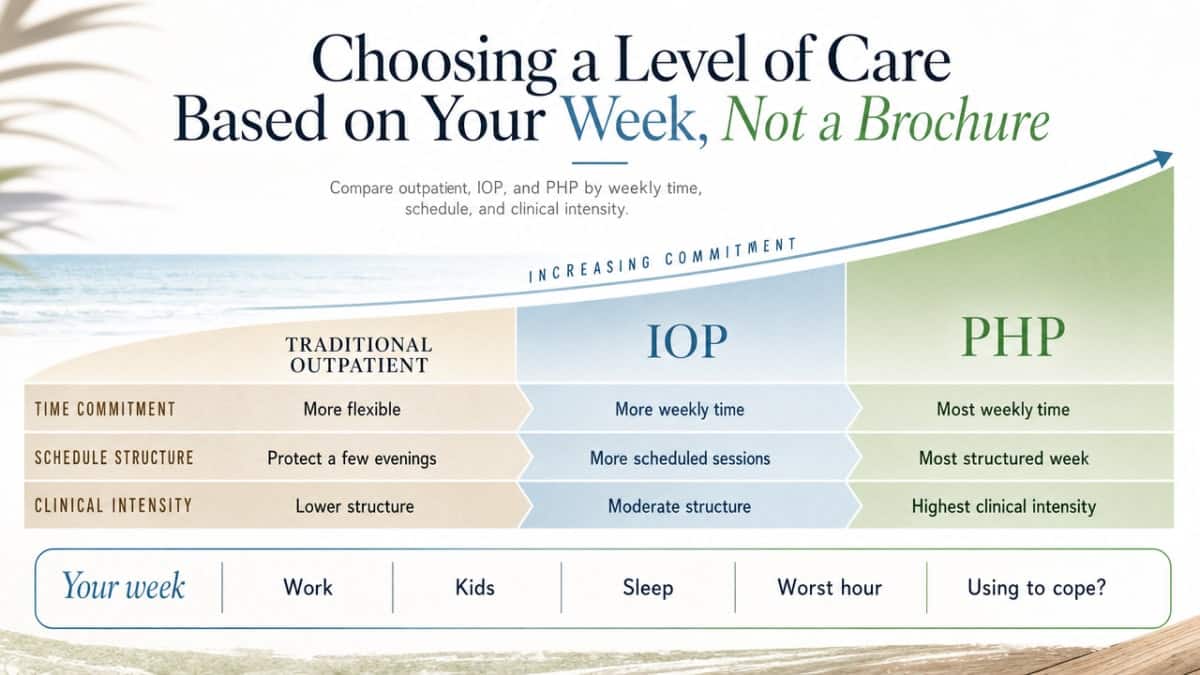
Choosing a Level of Care Based on Your Week, Not a Brochure
Most program pages explain levels of care as if you were comparing trim packages on a car. Outpatient. IOP. PHP. Each with a paragraph of features. That framing is backwards. The right question isn’t which program sounds most thorough. It’s how many hours your current week can actually hold, and how much structure your symptoms actually need.
So start with the honest inventory. How many evenings could you protect for treatment without your job or your kids quietly falling apart? How bad is the worst hour of your day right now? Are you sleeping? Are you using something to get through? The answers point you toward a level of care faster than any brochure will. Flexible outpatient mental health Orange County programs are built around three main tiers, and the differences between them are mostly about time and intensity, not quality.
Traditional Outpatient: One or Two Hours, Built Around Your Calendar
Traditional outpatient is what most people picture when they think of therapy. You meet with a therapist for fifty or sixty minutes, usually once a week, sometimes every other week. You might add a psychiatrist appointment every month or two for medication. Total time commitment: one to two hours a week, scheduled around your calendar.
This level fits if your symptoms are present but manageable, you’re sleeping most nights, and you’re not in a pattern that’s actively unraveling your work or your relationships. It’s also a reasonable step-down after a more intensive program. What it isn’t built for: a depression that’s getting heavier each month, panic attacks that have started showing up in meetings, or drinking that’s quietly escalated. If that’s where you are, one hour a week probably isn’t enough holding.
Intensive Outpatient (IOP) and Evening IOP: Treatment That Starts After Work
IOP is the level most working adults in Orange County end up needing, and most don’t know it exists in a form they can actually use. A standard IOP runs about nine to twelve hours a week, usually three days a week, three hours per session. Evening IOP shifts those sessions to roughly 6 to 9 p.m., which is the difference between treatment being theoretically available and treatment being something you can actually attend on a Tuesday.
Within that block you get group therapy, skills training (often DBT and CBT-based), individual sessions, and access to medication management. California’s DHCS recognizes outpatient as a distinct, licensed level of behavioral health care with its own standards 12, which is why a real IOP looks structurally different from weekly therapy, even when both happen in an office that looks like an office.
Evening IOP is the version that lets you keep your job, pick up your kid from practice, and still get clinical-grade treatment three nights a week. For most working adults reading this, that’s the level that fits for flexible outpatient mental health Orange County.
Partial Hospitalization (PHP): When You Need More Hours, Briefly
PHP is the most intensive outpatient level. You’re in programming roughly five to six hours a day, five days a week, usually during business hours. It’s structured like a full-time clinical day: group therapy, individual sessions, skills work, psychiatric care, sometimes family sessions. You still sleep at home.
PHP makes sense when symptoms are interfering significantly with daily functioning, when you’ve recently stepped down from a hospital stay, or when an IOP isn’t quite enough holding for what’s happening. The trade-off is real: at twenty-plus hours a week during the day, most people need short-term leave, FMLA, or a flexible employer to attend. That can feel daunting. But PHP is often only a few weeks, with a planned step-down to IOP, then traditional outpatient. It’s a sprint, not a season.
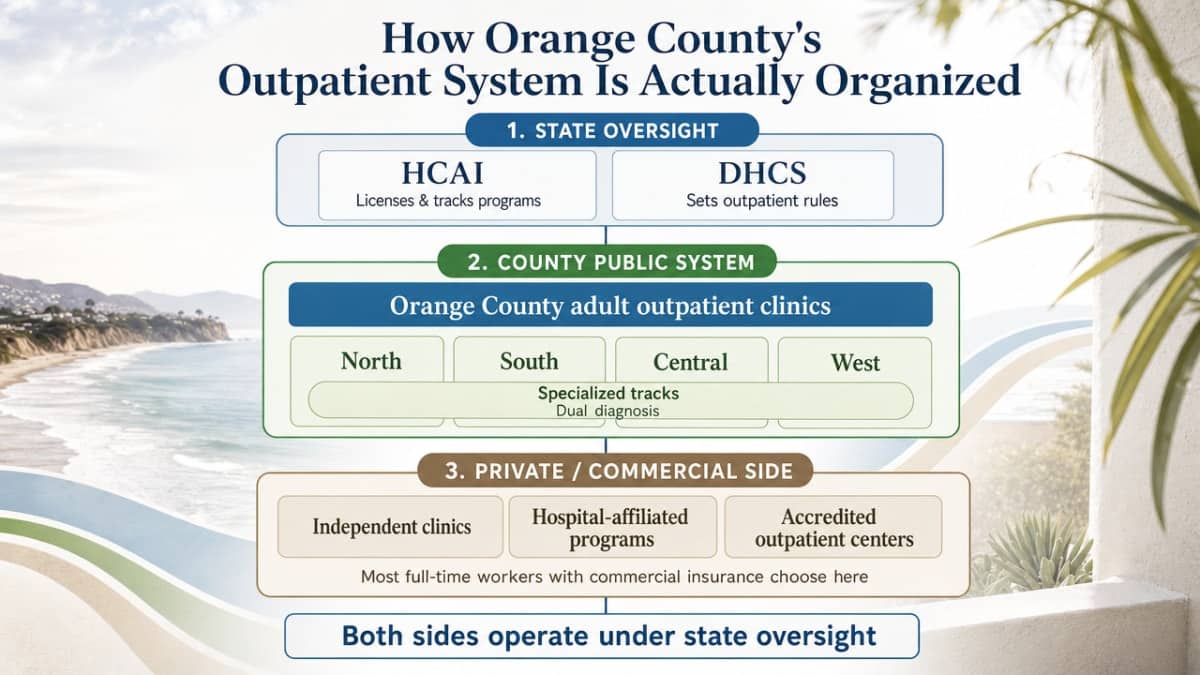
How Orange County’s Outpatient System Is Actually Organized
Orange County’s behavioral health landscape can feel opaque from the outside, but it follows a logic once you see the pieces. On the public side, the county organizes adult outpatient clinics by geographic region, roughly North, South, Central, and West, with specialized tracks for things like dual diagnosis layered on top. On the private and commercially insured side, a wider mix of independent clinics, hospital-affiliated programs, and accredited outpatient centers fills in the map. If you’re working full-time with commercial insurance, you’re mostly choosing among that second group.
What ties both sides together is state oversight. The California Department of Health Care Access and Information licenses and tracks outpatient behavioral health programs, and DHCS sets the rules outpatient providers have to follow on staffing, clinical standards, and service definitions 11. Outpatient programs that treat co-occurring substance use also work under a separate DHCS licensing and certification framework 12. That’s a long way of saying: a real IOP isn’t just a room with chairs. It’s a regulated level of care with documented standards behind it.
The bigger story right now is funding. For two decades, much of California’s community mental health work was paid for through the Mental Health Services Act, funded by a 1% tax on personal income above $1 million 4. That law is now transitioning into the Behavioral Health Services Act, which redirects funding toward people with the most significant needs, adds substance use disorder treatment as a covered priority, expands housing interventions, and grows the workforce 4. For Orange County, that shift is reshaping which flexible outpatient mental health Orange County programs get supported, where capacity is being added, and how integrated dual diagnosis care is being prioritized inside the public system.
The Therapies You Should Expect to See on the Schedule
When you look at an outpatient program’s weekly schedule, the acronyms can blur together. CBT on Monday. DBT skills group on Wednesday. EMDR available on request. Medication management every two weeks. The names matter less than what they’re actually doing for you. A credible flexible outpatient mental health Orange County program isn’t picking therapies off a menu. It’s matching specific evidence-based methods to the specific things you walked in struggling with, and then giving you enough repetition to make them stick.
Here’s what each of these is meant to do, and what you should expect to feel happening over the first few weeks.
CBT, DBT, and EMDR in Plain Language
Cognitive Behavioral Therapy is the workhorse. It targets the loop between what you think, what you feel, and what you do. If you spiral after a critical email and end the night three drinks in, CBT helps you catch the thought that started the cascade and test whether it’s actually true. It’s structured, skills-based, and usually shows results within weeks, not months.
Dialectical Behavior Therapy was built originally for people whose emotions move faster and bigger than they can manage. It’s now used widely for anxiety, depression, trauma responses, and the emotional volatility that often shows up alongside substance use. DBT teaches four concrete skill sets: mindfulness, distress tolerance, emotion regulation, and interpersonal effectiveness. In a group, you don’t just talk about a hard week. You learn a specific technique and practice it.
EMDR, or Eye Movement Desensitization and Reprocessing, is the one most people haven’t heard of until they need it. It’s used for trauma, including the kind you might not call trauma, the chronic background stress of a hard childhood or a job that broke you down for years. EMDR helps your brain reprocess memories that are still firing as if they’re happening now. Many people find it works when talk therapy alone hasn’t.
Medication Management Without the Pill-Mill Feel
For some conditions, therapy alone is enough. For others, including moderate to severe depression, certain anxiety disorders, bipolar disorder, and ADHD, medication is part of getting your footing back. A good outpatient program treats medication as one tool among several, not the whole answer and not an afterthought.
What that looks like in practice: you meet with a psychiatric provider, usually a psychiatrist or psychiatric nurse practitioner, who actually has time to ask about your history, your sleep, your other medications, and what you’ve tried before. Appointments are typically every two to four weeks at the start, then spaced out as things stabilize. They coordinate with your therapist so the medication conversation and the therapy work aren’t happening in separate universes.
If you’re tapering off something, including benzodiazepines or other medications that need careful step-downs, that happens under medical supervision with a plan, not a guess. The goal of medication management in a flexible outpatient mental health Orange County setting is the same as the goal of the rest of the program: give you enough support to do the work, without making you dependent on the support itself.
When Anxiety, Depression, or Trauma Overlaps With Substance Use
A pattern shows up often in working adults who finally walk into an intake: the anxiety came first, or the depression did, or something happened years ago that never got processed. Drinking, or a benzodiazepine prescription that crept up, or weed at the end of every night, started as a way to get some relief. It worked, for a while. Then it stopped working, and it started costing you something.
If that’s close to your situation, the most important thing to know is that treating one without the other rarely holds. A systematic review of integrated care for concurrent mental health and substance use disorders found that integrated outpatient models tend to produce more effective outcomes on both fronts than treating the two conditions in separate places with separate teams 6. When your therapist knows about the wine, and your prescriber knows about the panic, and the group on Wednesday addresses both, the work compounds. When you have to tell three different providers three versions of your story, things fall through the cracks. That’s not a character flaw. It’s a system design problem.
Flexible outpatient mental health Orange County programs that specialize in co-occurring care are built to handle both sides in one place. That usually means a clinical team trained in dual diagnosis, group content that names substance use without shame, medication management that accounts for what you’ve been using, and a treatment plan that doesn’t ask you to pick which problem to solve first.
One language note worth making here. You are not your diagnosis, and you are not your substance use. A person living with depression who also drinks too much is a person, not a label. Good flexible outpatient mental health Orange County programs talk about you that way too. If a provider doesn’t, that tells you something about the place before you’ve signed anything.
Access, Insurance, and How Quickly You Can Actually Start
One of the quieter reasons people put off care is the assumption that getting in will take weeks. Calls to play, voicemails to leave, forms to fill out at midnight. Sometimes it does take a while. Often, it doesn’t.
Most flexible outpatient mental health Orange County programs run a phone-based intake that takes thirty to forty-five minutes. You talk through what’s been happening, what you’ve tried, what your week actually looks like, and what insurance you have. If you’re a good fit clinically, many programs can schedule a full assessment within a few business days and start you in group the following week. Evening IOP cohorts often have rolling admissions, which means you’re not waiting for a session to begin.
If you have commercial insurance through a major carrier, your flexible outpatient mental health Orange County benefits are likely stronger than you think. Federal parity rules require that behavioral health coverage be comparable to medical and surgical coverage, and California’s network adequacy standards require plans to maintain outpatient providers within specific time-and-distance ranges of where you live 13. A reputable program will verify your benefits before your first session and tell you what’s covered, what isn’t, and what your authorization looks like. You should not have to guess.
A few practical things to ask on that first call:
- Is the program in-network with your insurer?
- Do they offer evening IOP, or only daytime?
- Is dual diagnosis treated in the same program, or referred out?
- How soon can you start?
The answers are quick, and they tell you a lot.
The Honest Part: Stigma, Time, and Starting Anyway
Here’s the part most program pages skip. Reaching out is the hard part. Most people put it off for months, sometimes years, not because they don’t know they need help, but because of three quiet barriers that nobody names out loud.
The first is being seen. You’re worried about pulling into the parking lot and recognizing someone from your kid’s school, or someone from work. That fear is real, and it’s also smaller than it feels. Outpatient offices in Orange County are usually in unmarked professional buildings. Nobody at the front desk says your business out loud. The person you might worry about running into is, statistically, more likely to be there for the same reason you are.
The second is time. You’re already running on fumes, and the idea of adding nine more hours a week to your schedule sounds impossible. It is hard. It’s also temporary in its most intensive form. Most people in evening IOP attend for eight to twelve weeks at the higher intensity, then step down. You are not signing up for a forever commitment. You’re borrowing time from a depleted version of yourself to give it back to a sturdier one.
The third is guilt. The voice that says other people have it worse, that you should be able to handle this, that taking treatment time is selfish when your team is short-staffed or your kids need you. That voice is not telling you the truth. Untreated anxiety, depression, and trauma do not stay quietly contained. They show up in your patience, your sleep, your marriage, your judgment. Treating them is not taking away from the people who count on you. It is one of the more direct ways to actually show up for them.
You don’t have to be in crisis to deserve care. You don’t have to have a label yet. You don’t have to know which level of flexible outpatient mental health Orange County program is right before you call. That’s what the intake conversation is for. Programs like 449 Recovery exist to help you figure out what fits, start where you actually are, and keep your life intact while you do the work. The first call is the hardest one. After that, you’re already moving.
Frequently Asked Questions
Can I keep working full-time while in an outpatient mental health program in Orange County?
Yes, and that’s the point of the model. Evening IOP runs roughly three nights a week, often 6 to 9 p.m., so you can work a full day and still attend. Traditional outpatient is even lighter. PHP is the exception: it usually requires daytime hours and short-term leave. Most working adults who choose flexible outpatient mental health Orange County programs keep their jobs throughout treatment.
What is the difference between IOP and PHP, and how do I know which one I need?
IOP runs about nine to twelve hours a week, often three evenings. PHP runs roughly five to six hours a day, five days a week, during business hours. PHP fits when symptoms are interfering significantly with daily functioning or when you’re stepping down from a hospital stay. A clinical intake assessment will tell you honestly which level matches what’s happening, rather than asking you to guess from a website.
Does insurance cover outpatient mental health in Orange County?
In most cases, yes. Federal parity rules require behavioral health coverage comparable to medical coverage, and California enforces network adequacy standards on plans covering flexible outpatient mental health Orange County services 13. Major commercial carriers typically cover IOP, PHP, and traditional outpatient when medically necessary. A program’s intake team should verify your benefits before your first session and explain what’s authorized.
What therapies should I expect in an outpatient mental health program?
Expect a mix of evidence-based methods matched to what brought you in. CBT for thought-feeling-behavior loops. DBT for emotion regulation and distress tolerance. EMDR when trauma is part of the picture. Group therapy several times a week, individual sessions weekly or biweekly, and medication management when needed. A credible flexible outpatient mental health Orange County program coordinates these so they reinforce each other rather than running in parallel silos.
What if I’m dealing with both a mental health condition and substance use?
Look for an integrated dual diagnosis program rather than two separate providers. A systematic review of integrated care for concurrent disorders found that integrated models tend to be more effective than treating each condition in isolation 6. In practice, that means one clinical team addressing your depression or anxiety and your substance use in the same building, on the same treatment plan, without asking you to choose which problem to solve first.
How quickly can I actually start outpatient mental health treatment?
Faster than most people expect. A phone intake usually takes thirty to forty-five minutes. From there, many flexible outpatient mental health Orange County programs can schedule a full assessment within a few business days and place you in a group the following week. Evening IOP cohorts often have rolling admissions, so you’re not waiting for a new session to begin. Ask about start dates on your first call.
References
- Orange County Aggregate Report – Specialty Mental Health Services (Children and Youth). https://www.dhcs.ca.gov/services/MH/Documents/30-Orange_CtyAggRep-ADA.pdf
- Health Care Almanac – Charts and Statistics (Mental Health in California). https://www.senate.ca.gov/sites/senate.ca.gov/files/mentalhealthalmanac_2022_charts_and_stats.pdf
- Assisted Outpatient Treatment Program – DHCS. https://www.dhcs.ca.gov/formsandpubs/Pages/Assisted-Outpatient-Treatment-Program.aspx
- Mental Health Services Act (MHSA) / Behavioral Health Services Act (BHSA) – DHCS. https://www.dhcs.ca.gov/services/MH/Pages/MH_Prop63.aspx
- Medi-Cal Behavioral Health Fee Schedules Fiscal Year 2025-26. https://www.dhcs.ca.gov/services/MH/Pages/Fiscal-Year-2025-26-Medi-Cal-Behavioral-Health-Fee-Schedules-FY25-26.aspx
- A Review of Integrated Care for Concurrent Disorders. https://pubmed.ncbi.nlm.nih.gov/30806190/
- Evaluating Integrated Care: Review of Results from Literature. https://www.macpac.gov/publication/evaluating-integrated-care-review-of-results-from-literature/
- Systematic review of the effectiveness of integrated care pathways. https://www.academia.edu/130475634/Systematic_review_of_the_effectiveness_of_integrated_care_pathways
- QuickFacts: Orange County, California. https://www.census.gov/quickfacts/fact/table/orangecountycalifornia/PST045224
- Hospital and Workforce Behavioral Health Data in California – HCAI. https://hcai.ca.gov/data/initiatives/behavioral-health/
- Behavioral Health Services – DHCS – CA.gov. https://www.dhcs.ca.gov/services/Pages/BHS.aspx
- Residential and Outpatient – DHCS – CA.gov. https://www.dhcs.ca.gov/provgovpart/Pages/Residential_and_Outpatient.aspx
- Mental Health Plan Final Rule and Parity Information – DHCS. https://www.dhcs.ca.gov/services/Pages/Mental-Health-Plan-Final-Rule-and-Parity-Information.aspx
- Integrated vs non-integrated treatment outcomes in dual diagnosis: a systematic review. https://pmc.ncbi.nlm.nih.gov/articles/PMC10157410/



