Key Takeaways
- An Orange County evening IOP runs 9 to 19 clinical hours per week under ASAM Level 2.1, structured around working adults with groups after hours and on weekends 4.
- For most working professionals who can stay safe at home, intensive outpatient care matches inpatient outcomes when programs deliver real clinical hours led by licensed clinicians 9.
- Integrated dual-diagnosis treatment, with one team handling anxiety, depression, and substance use together, outperforms parallel referrals and should be confirmed before enrolling 8.
- Before committing, compare licensure, the clinical team’s credentials, named modalities like CBT, DBT, EMDR, and contingency management, individualized treatment planning, and a written step-down plan 12, 3.
What an evening IOP actually asks of a working adult
You already know what your week looks like. Back-to-back meetings, a commute up the 405 or the 5, a partner or kids who need you present, and somewhere underneath all of it, the part you haven’t said out loud yet: the anxiety that won’t quit, the drinking that crept up, the depression that’s been wearing a smile for months. So when you start researching an orange county intensive outpatient program, you’re not really asking what IOP is. You’re asking whether it can fit inside a life that’s already full.
Here’s the honest answer. An orange county intensive outpatient program is more demanding than weekly therapy and lighter than residential care. In California, it’s a defined clinical level of treatment, typically delivered in the evenings for working adults, with group therapy, individual sessions, psychoeducation, and relapse prevention built into a structured weekly schedule 1. You keep your job. You sleep in your own bed. You also commit several evenings a week to doing real clinical work.
That tradeoff is the point. For many professionals managing anxiety, depression, trauma, or co-occurring substance use, an evening IOP is the level of care that actually matches the problem without forcing a career pause. It asks for hours, not your whole life. It asks for honesty in a group room, not a leave of absence. And if you’ve been quietly carrying this for a while, the fact that you’re reading this is already a step. The rest of this guide walks through what to expect, what to ask, and how to tell a serious program from a slick one.
What qualifies as intensive outpatient care in California
ASAM Level 2.1 and the 9 to 19 hour weekly range
If you’re trying to figure out whether what you’re looking at online is actually an orange county intensive outpatient program or just weekly therapy with a fancy name, the simplest test is hours. In California, intensive outpatient treatment is defined as ASAM Level 2.1 care, which requires a minimum of 9 and a maximum of 19 hours of services per week 4. That range is the structural backbone. Anything less is standard outpatient. Anything more is partial hospitalization.
Those hours aren’t arbitrary. They reflect a clinical floor: enough contact time to do real therapeutic work, build group cohesion, and address co-occurring symptoms, without pulling you out of your home or job. For a working adult, that usually translates to three group sessions a week, plus an individual therapy session and a psychiatric or medication management appointment depending on what you need.
What’s inside those hours matters as much as the total. A credible orange county intensive outpatient program uses that time for group therapy, individual sessions, psychoeducation, family work, and relapse prevention 1. You shouldn’t be sitting through nine hours of generic lectures or watching videos. You should be doing structured clinical work led by licensed clinicians, with treatment goals you can name out loud.
The hour range also gives you a useful question to ask any program you call: “How many clinical service hours per week, and what’s the mix?” A program that can answer cleanly is operating inside the standard. A program that dodges the question, or pads the schedule with non-clinical activities to hit a number, is telling you something. You’re allowed to ask. In fact, asking is one of the first signs you’re treating your recovery the way you’d treat any other serious decision in your life.

How IOP sits between PHP and standard outpatient
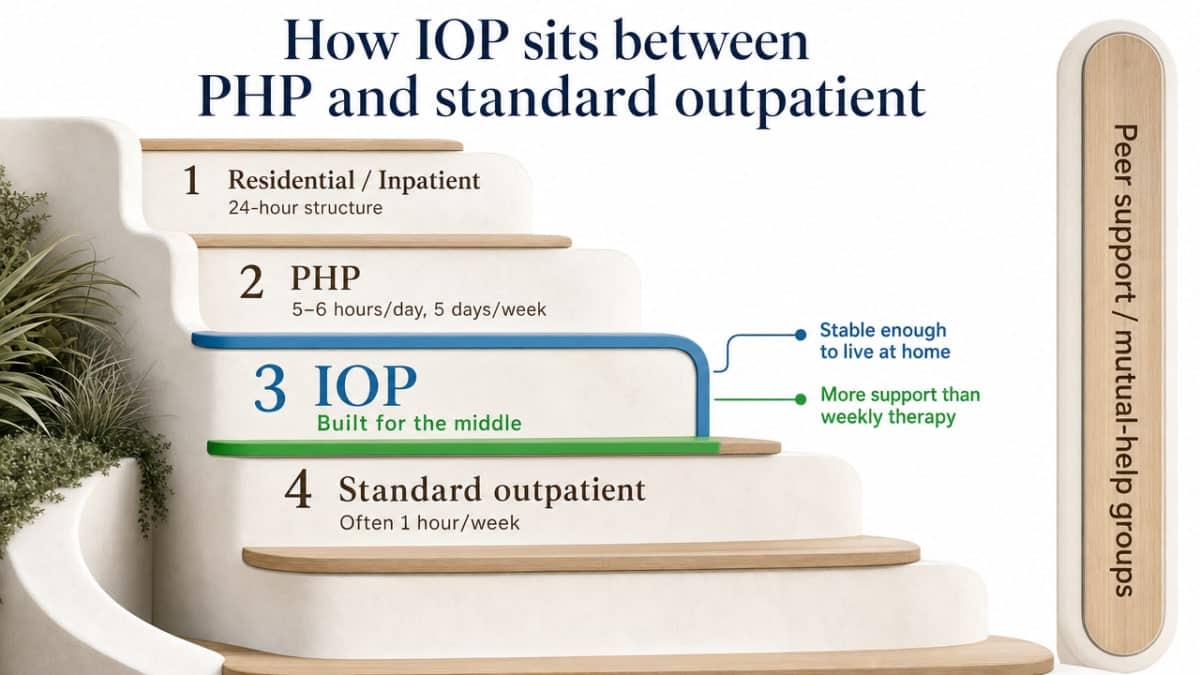
Picture the continuum of care as a staircase, not a menu. At the top, residential and inpatient settings provide 24-hour structure for people who can’t be safe or stable at home. A step down from there is partial hospitalization, or PHP, which typically runs five or six hours a day, five days a week, and looks a lot like a part-time job in itself. Below PHP sits intensive outpatient. Below that, standard outpatient therapy, often an hour a week. And running alongside all of it, peer support and mutual-help groups 2.
An orange county intensive outpatient program is built for the middle. You’re stable enough to live at home, get yourself to sessions, and hold most of your responsibilities, but the symptoms or the substance use are loud enough that a single hour of therapy each week isn’t moving the needle. That’s the gap IOP fills.
The staircase also explains why so many people enter an orange county intensive outpatient program after a higher level of care, or step down into it from PHP. The clinical research is clear that people who continue treatment after an intensive phase, rather than stopping cold, have better long-term outcomes 2. So IOP isn’t always the starting point. Sometimes it’s the bridge between a more intensive episode and the regular outpatient therapy you may stay in for a year or longer.
Knowing where IOP sits on the staircase helps you ask the right question when you call a program: not “do you treat anxiety” or “do you treat substance use,” but “what level of care do you think I need, and why?” A program willing to recommend up or down, instead of just selling you the slot they have open, is a program worth your time.
Why outpatient intensity can be clinically enough
The fear sitting underneath your research is probably this: if you don’t take a leave of absence, if you don’t disappear to a facility for thirty days, are you really getting serious treatment? It’s a fair worry. The cultural image of recovery is still a sun-drenched campus and a packed suitcase. So when you start comparing that picture to an orange county intensive outpatient program where you sleep at home and go to work the next morning, the math feels off.
The evidence says the math works. A systematic review of substance abuse intensive outpatient programs concluded that well-designed IOPs are as effective as inpatient and residential treatment for most individuals with substance use disorders, with programs typically providing at least 9 hours of services per week 9. That’s not a marketing claim from a treatment center. That’s a peer-reviewed comparison across multiple studies, looking at the same outcomes you care about: reduced use, sustained recovery, improved functioning.
For working adults with anxiety, depression, or co-occurring substance use who are functional enough to keep showing up to their lives, an orange county intensive outpatient program isn’t a compromise. It’s the level of care the research actually supports. The intensity comes from what happens in the room, not from whether you sleep there.
A realistic week inside an evening IOP
Let’s get specific, because vague schedules are how you talk yourself out of starting. A typical evening orange county intensive outpatient program builds the week around three group sessions plus an individual therapy hour, with a psychiatry or medication appointment layered in as needed. That’s the shape. The hours land after work, not during it.
One real-world model worth looking at: an academic medical center program runs its intensive outpatient groups on Tuesday and Thursday evenings and Saturdays, deliberately scheduled around full-time employment 6. Translate that to your own week and it might look like this. Monday is a regular workday. Tuesday you leave the office at 5:30, grab something to eat in the car, and sit in group from 6 to 9. Wednesday is yours. Thursday is another 6 to 9 group. Friday you have your individual therapy session, maybe at lunch or right after work. Saturday morning you do a third group, often skills-focused, and you still have the rest of the weekend with your family.
What happens inside those evening hours is the actual treatment. Process group, where you talk about what came up that week. Skills group, where you learn and practice CBT or DBT tools. Psychoeducation, where you understand what’s happening in your brain and your patterns. Relapse prevention planning. Some weeks include a family session if a partner or parent is part of the picture.
The honest part: the first two weeks feel hard. You’re tired from work, you’d rather go home, and group therapy is uncomfortable until it isn’t. By week three, most people in an orange county intensive outpatient program start to notice something shifting. The Tuesday and Thursday slots stop feeling like an obligation and start feeling like the part of the week that holds the rest of it together. You’re not adding stress to your life. You’re finally giving the hardest part of it a place to go.
Dual diagnosis as the default, not the upgrade
Why integrated care outperforms parallel tracks
Here’s something most program websites won’t say out loud: if you’re dealing with both anxiety and drinking, or depression and pills, or trauma and any of it, treating those things in separate rooms with separate clinicians is the slow path. For a long time, that’s exactly how the system was built. You’d see a therapist for the depression. You’d go to a different group for the substance use. The two clinicians wouldn’t talk. You’d be the one trying to hold both stories together while exhausted from holding everything else.
An integrated orange county intensive outpatient program treats the two as one clinical picture, because that’s what they actually are. The anxiety drives the drinking. The drinking worsens the anxiety. The trauma feeds both. Federal treatment guidance has been clear for years that matching the intensity of services to client needs means addressing co-occurring conditions inside the same program, not punting one of them down the hall 1.
The client-experience evidence backs this up. A 2025 peer-reviewed study of an integrated intensive outpatient program for adults with substance use and co-occurring mental disorders reported high levels of satisfaction along with improvements in both substance-related and psychological symptoms 8. People in those programs didn’t feel like they were juggling two diagnoses. They felt like one team was working on one person.
When you call an orange county intensive outpatient program, the question to ask isn’t “do you treat dual diagnosis.” Most will say yes. The better question is, “who’s coordinating my mental health and substance use treatment, and how often do they actually talk?” If the answer is one clinical team, one treatment plan, and weekly case review, you’re looking at integrated care. If it’s two referrals and a coordination promise, keep looking.
Evidence-based modalities to expect: CBT, DBT, EMDR, contingency management
You don’t need to become a clinician to vet an orange county intensive outpatient program, but you do need to know the names of the therapies that actually work. The four worth memorizing are CBT, DBT, EMDR, and contingency management. If a program can’t tell you which of these they use and why, that’s information.
Cognitive behavioral therapy, or CBT, is the workhorse. It’s the most studied talk therapy for substance use disorders, and a major review concluded it has strong empirical support across multiple substances 12. CBT is also one of the most effective treatments for anxiety and depression, which is why it shows up in nearly every credible dual-diagnosis program. You learn to spot the thoughts that drive the spiral, test them against reality, and replace the behaviors that keep the cycle going.
Dialectical behavior therapy, or DBT, was originally built for emotional regulation and is especially useful if you struggle with intense mood swings, self-harm urges, or relationships that feel like wildfires. The skills modules, like distress tolerance and interpersonal effectiveness, translate directly into the meetings, family dinners, and Sunday-night dread that fill a working adult’s week.
EMDR, eye movement desensitization and reprocessing, is the trauma piece. If your anxiety or substance use has roots in something that happened to you, EMDR is the modality designed to help your nervous system actually process it, not just talk around it.
Contingency management is the one most people haven’t heard of. It’s a structured incentive approach, and a trial in dual-diagnosis clients found it significantly increased both treatment attendance and drug-free days when added to an intensive outpatient program 3. Not every orange county intensive outpatient program uses it, but the fact that it works tells you something about what an evidence-based program can include. Ask. The answers will tell you whether the program is built on research or vibes.
Vetting an Orange County intensive outpatient program
You’ve narrowed it down to a few options. The websites all use similar words: compassionate, evidence-based, holistic. The intake coordinators are warm on the phone. So how do you actually tell which orange county intensive outpatient program is built around clinical care and which one is built around a sales funnel? You ask better questions than they’re prepared for.
Start with licensure and accreditation. In California, an outpatient mental health and substance use program should be licensed or certified by the Department of Health Care Services, and the strongest programs also carry CARF or Joint Commission accreditation. These aren’t marketing badges. They mean an outside body has reviewed clinical documentation, staff credentials, and treatment planning. If a program can’t tell you who licenses them in 30 seconds, that’s your answer.
Next, ask about the clinical team. Who runs the groups? Are they licensed clinicians (LMFTs, LCSWs, psychologists), or are they peer counselors leading therapeutic groups they aren’t credentialed for? Is there a psychiatrist on staff for medication management, or is psychiatry an outside referral you’re left to chase down? An orange county intensive outpatient program serious about dual diagnosis will have prescribers and licensed therapists working as one team, not stitched together after intake.
Then push on the modalities. The earlier section named the ones that matter: CBT, DBT, EMDR, and structured incentives like contingency management 12, 3. Ask which ones the program actually delivers, how often, and who’s trained in them. “We use a blend” is not an answer. “Our Tuesday group is CBT-based, Thursday is DBT skills, individual sessions use EMDR for trauma when indicated” is an answer.
Ask about treatment planning. Federal guidance is explicit that intensity should be matched to client needs, with individualized goals, not a standard curriculum everyone rotates through 1. A serious program will describe how your treatment plan gets built in the first week, who reviews it, and how often it changes. If the answer sounds like a fixed 12-week track regardless of what you walk in with, you’re looking at a product, not a clinical program.
Finally, ask about outcomes and step-down. What percentage of clients complete the program? What does aftercare look like, and is it included or sold separately? An orange county intensive outpatient program that can talk plainly about completion rates, continuing care, and what happens in month three is one that’s thinking about your recovery, not just your admission.
Step-down and continuing care after IOP
The day you finish an orange county intensive outpatient program is not the finish line. It’s the handoff. And how that handoff is planned matters more than most people realize when they’re still in the thick of week four or five, just trying to make it to Thursday’s group.
Federal treatment guidance is direct about this. People who step down from intensive outpatient treatment into ongoing outpatient care and structured continuing care have better long-term substance use outcomes than people who simply terminate after the intensive phase ends 2. The drop-off is the danger zone. You’ve built momentum, learned skills, found a rhythm, and then suddenly your Tuesday and Thursday evenings are empty again. Without something to step into, the old patterns have an open lane.
A meta-analysis of continuing care interventions across multiple studies found small but significant positive effects on substance use outcomes over time 13. “Small but significant” isn’t a marketing line. It’s researcher language for: this consistently helps, across many designs, for many people. The effect compounds the longer you stay engaged.
So when you’re vetting an orange county intensive outpatient program, ask what comes next before you ever start. A real step-down plan includes weekly or bi-weekly outpatient therapy, ongoing psychiatric follow-up if you’re on medication, an alumni or aftercare group that meets regularly, and a written relapse prevention plan you helped build. Mutual-help meetings, whether 12-step, SMART Recovery, or peer support, often fit in here too.
If a program treats discharge as a calendar date instead of a transition, keep looking. The orange county intensive outpatient program worth your time will already be talking about month six during week six.
Making the first call without disrupting your career
The hardest part isn’t the program. It’s the dial. You’ve researched, you’ve read, and now there’s a phone number sitting in a tab waiting for you to do something about it. So here’s what helps. You don’t have to tell your employer anything to make the first call. You don’t have to take a day off to do intake. An orange county intensive outpatient program is built around the assumption that you’re working, which means evening and weekend slots exist precisely so you can keep your schedule intact while you start 6.
When you call, you’re not committing. You’re asking questions. How many hours per week, and at what times? Who’s on the clinical team? Is mental health and substance use handled by one integrated team? What does the first two weeks actually look like? A good intake coordinator will hear the working-adult subtext and answer plainly.
If confidentiality is on your mind, federal privacy rules protect what you share, and most professionals find that the FMLA, EAP, or simply scheduling around existing personal time is enough to start treatment without anyone at work needing details. The call itself is the win. Everything else gets built from there.
Frequently Asked Questions
How many hours per week does an Orange County intensive outpatient program require?
In California, an orange county intensive outpatient program is defined as ASAM Level 2.1 care, which requires a minimum of 9 and a maximum of 19 hours of clinical services per week 4. For most working adults, that lands as three evening group sessions plus an individual therapy hour, with a psychiatry appointment added when medication management is part of the plan.
Can I keep working full-time while attending an evening IOP?
Yes, and that is the design intent. Evening and weekend IOP models exist precisely so adults with full-time jobs can stay employed during treatment, with groups scheduled in the evenings and on Saturdays 6. You commit several weeknights and usually one weekend morning. Most clients in an orange county intensive outpatient program do not take leave from work, though some choose to use FMLA or PTO for the first week.
Is intensive outpatient care really enough if I have both anxiety and a substance use issue?
For most adults who can stay safe at home, yes. A 2025 study of integrated intensive outpatient treatment for substance use and co-occurring mental disorders reported high client satisfaction and improvements in both substance-related and psychological symptoms 8. The key word is integrated. An orange county intensive outpatient program that treats anxiety and substance use as one clinical picture with one team gives you a better shot than parallel tracks.
What therapies should a credible Orange County intensive outpatient program offer?
At minimum, look for cognitive behavioral therapy, which has strong empirical support for substance use disorders and is a core modality in serious programs 12. Dialectical behavior therapy for emotional regulation and EMDR for trauma should also be on the menu. Some programs add contingency management, an evidence-based incentive approach shown to improve attendance and drug-free days in dual-diagnosis clients 3. Ask which clinicians are trained in each.
What happens after I finish an intensive outpatient program?
You step down, you do not stop. Federal guidance and a meta-analysis of continuing care both show that ongoing, lower-intensity services after the intensive phase produce better long-term substance use outcomes than ending treatment cold 2, 13. A real aftercare plan from an orange county intensive outpatient program includes weekly outpatient therapy, psychiatric follow-up if needed, an alumni group, and a written relapse prevention plan you helped build.
How do I tell a clinically serious IOP from a marketing-heavy one?
Ask questions a sales script cannot answer. Who licenses you, and what is your accreditation? Who runs the groups, and are they licensed clinicians? How are mental health and substance use treatment coordinated? Federal guidance is clear that intensity should be matched to individual client needs with personalized treatment planning 1. An orange county intensive outpatient program that gives specific, named answers about modalities and clinicians is the one worth your time.
References
- TIP 47: Substance Abuse: Clinical Issues in Intensive Outpatient Treatment. https://www.samhsa.gov/resource/ebp/tip-47-substance-abuse-clinical-issues-intensive-outpatient-treatment
- Chapter 3. Intensive Outpatient Treatment and the Continuum of Care. https://www.ncbi.nlm.nih.gov/books/NBK64088/
- Contingency Management for Patients with Dual Disorders in Intensive Outpatient Treatment for Addiction. https://pmc.ncbi.nlm.nih.gov/articles/PMC4292935/
- Intensive Outpatient Treatment and the Drug Medi-Cal Organized Delivery System: Frequently Asked Questions. https://www.dhcs.ca.gov/provgovpart/Documents/DMC-ODS_Waiver/DMC_ODS_IOT_FAQ_06.18.pdf
- OC Community Health Improvement Plan 2024–2026. https://healthpolicy.ucla.edu/our-work/publications/oc-community-health-improvement-plan-2024-2026
- Intensive Outpatient and Outpatient Substance Use and Co-Occurring Treatment Program. https://www.med.upenn.edu/recovery/intensive-outpatient-and-outpatient-substance-use-and-co-occuring-treatment-program.html
- Drug Medi-Cal Organized Delivery System Overview (SUPT-03-01). https://dhs.saccounty.gov/BHS/Documents/BHS-Policies-and-Procedures/PP-BHS-SUPT-03-01-DMC-ODS-Overview.pdf
- Clients’ Experiences and Satisfaction with an Integrated Intensive Outpatient Treatment for Substance Use and Co-Occurring Disorders. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11898248/
- Substance Abuse Intensive Outpatient Programs: Assessing the Evidence. https://pmc.ncbi.nlm.nih.gov/articles/PMC4152944/
- Behavioral Health Program Performance Data (California CHHS). https://data.chhs.ca.gov/dataset/behavioral-health-program-performance-data
- Screening and Transition of Care Tools for Medi-Cal Mental Health Services. https://www.dhcs.ca.gov/screening-and-transition-of-care-tools-for-medi-cal-mental-health-services/
- Cognitive-Behavioral Therapy for Substance Use Disorders. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3016695/
- The Effectiveness of Continuing Care for Substance Use Disorders: A Meta-Analysis. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5757447/



