Key Takeaways
- Evening IOP tracks in Orange County preserve roughly nine clinical hours per week by running 6 to 9 p.m. blocks, so full-time work and family schedules stay intact 1.
- Research shows IOPs perform as effectively as inpatient care for most appropriate patients, and telehealth-blended formats match in-person retention while reducing the 405 commute problem 1, 6.
- Working professionals usually arrive with co-occurring anxiety, trauma, or depression alongside substance use; integrated programs treating both together produce stronger outcomes than parallel silos 5.
- Compare programs on group start and end times, whether hybrid delivery is built-in versus backup, integrated dual diagnosis under one plan, and confidentiality protections under HIPAA and 42 CFR Part 2.
Your Week, Not a Watered-Down Rehab
You already know what IOP stands for. You’ve already read the levels-of-care explainer on five different sites. What you actually need to know is whether iop treatment Orange County clinicians offer can hold up around a 9-to-6, two kids, and a commute that eats ninety minutes a day.
The short answer: yes.
Intensive outpatient programs were not invented as a softer alternative for people who couldn’t “commit” to real treatment. They were built as a distinct level of care, and the research backs them up. A systematic review of 12 studies found that IOPs produce substantial reductions in alcohol and drug use and perform as effectively as inpatient treatment for most individuals who need this level of care 1. That is a meaningful claim, drawn from substance use disorder cohorts, and it changes the math on what “stepping into treatment” has to cost you professionally.
Here is what this article is going to do, and what it is not.
It is not going to define IOP from scratch. You can recognize DBT, CBT, and EMDR on a program page. You know the difference between PHP and IOP in broad strokes. You are weighing a real decision about your calendar, your job, and your family — not a vocabulary quiz.
What you will get instead: the time architecture of evening and hybrid tracks, what the evidence says about telehealth-blended care, how dual diagnosis programming actually works inside a single week, and the conversations with HR and your manager that you are probably running in your head right now.
This is your week. Not a watered-down rehab.
What ‘Flexible’ Actually Means Clinically
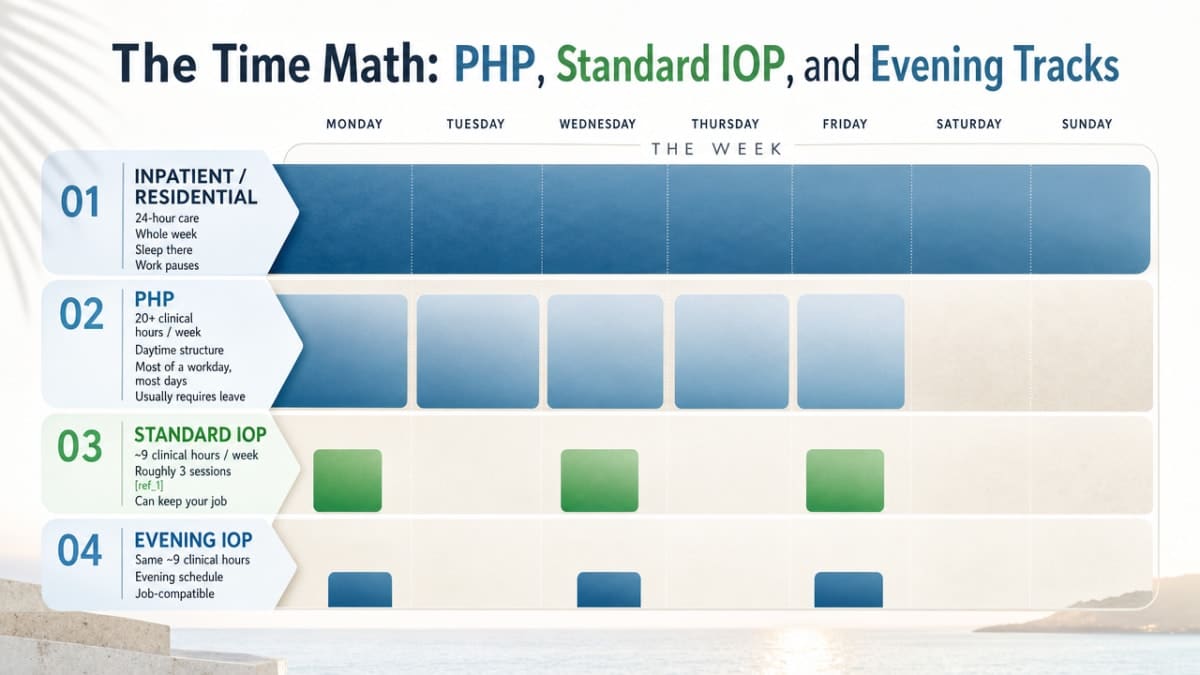
The Time Math: PHP, Standard IOP, and Evening Tracks
Let’s put numbers on your calendar before we put feelings on them.
Inpatient and residential care take your whole week. You sleep there. Work pauses. That is the entire point of that level of care, and for some people it is exactly right.
A partial hospitalization program (PHP) generally runs around 20 or more clinical hours per week — think most of a workday, most days. It is daytime structure for people who need close support but not 24-hour care. Most working adults cannot make a PHP fit without using leave.
A standard intensive outpatient program lands around nine clinical hours per week, spread across roughly three sessions 1. That is the number the evidence base keeps coming back to, and it is the number that lets iop treatment Orange County programs argue, credibly, that you can keep your job.
An evening IOP holds that same ~9-hour weekly dose but loads it into 6 to 9 p.m. blocks, Monday through Thursday or similar. The clinical content does not shrink. The clock just moves.
Here is what that means for your Tuesday.
You work your regular hours. You eat something quick. You drive (or log in). You sit in group from 6 to 9. You go home. You sleep in your own bed. Wednesday, you do your job again.
That is the architecture. Not less treatment — different timing. The clinical hours are real hours, doing real work.
What “flexible” should mean to you in iop treatment Orange County programs is not “easier.” It means the schedule is engineered so you can actually finish what you start.
Why Evening and Hybrid Formats Are an Evidence Decision
You are probably suspicious of virtual care. Reasonable. A lot of people are.
The instinct goes: if I am doing this remotely, I am doing a lesser version of it. Cheaper for them, easier for me, weaker for my recovery.
The data does not support that instinct — at least not in the way you are framing it.
One study of telehealth-delivered IOP for substance use disorders reported that treatment retention and abstinence outcomes did not significantly differ between virtual and in-person cohorts 6. People stayed in treatment at similar rates. Their substance use outcomes tracked similarly. The screen did not, in that sample, hollow out the work.
That is exactly why credible iop treatment Orange County programs lean hybrid — some on-site, some remote — rather than picking a side.
And there is a second reason to take telehealth-blended formats seriously, beyond outcomes. Engagement research on telehealth IOP for substance use disorders points out that virtual options reduce geographic and logistical barriers — meaningful in a county where a 4:45 p.m. group start would cost you two hours on the 405 3. The 6 p.m. group you can actually attend, on a screen from your kitchen on a Thursday, is clinically stronger than the in-person group you keep missing.
That is the evidence decision behind evening and hybrid iop treatment Orange County programs. Not a convenience. A retention strategy.
If you have been quietly waiting for someone to tell you it is allowed to do this from a laptop after work, here it is: the format is not the compromise. The format is what lets you finish.
Is IOP Actually Enough When You’re Working Full Time?
This is the question you keep circling, isn’t it.
If you can keep working, keep parenting, keep showing up to the 9 a.m. standup — is what you’re getting actually treatment, or is it a placeholder until you eventually have to take real leave?
Real answer: for most people in your situation, it is treatment. Not a placeholder.
The systematic review of substance abuse intensive outpatient programs — twelve studies, varied settings, varied populations — concluded that IOPs produce substantial reductions in alcohol and drug use and perform as effectively as inpatient treatment for most individuals who need this level of care 1. The scope matters here. That finding sits inside substance use disorder cohorts. It does not say every person with every condition belongs in IOP. It says that when IOP is clinically appropriate, the outcomes hold up against the higher-acuity option.
That is a different sentence than “IOP is good enough.” It is closer to: when this level of care matches your clinical picture, the calendar you keep is not the thing that decides whether you recover.
What does decide it: showing up. Doing the work in the room. Practicing the skills between sessions.
The honest caveat. IOP is not enough if you need medical detox, if your safety is acute, or if your symptoms are pulling you under faster than weekly sessions can stabilize. A good intake for any iop treatment Orange County program will tell you that directly. If PHP or a higher level of care is the right starting point, the clinician should say so — and then step you down to IOP when you are ready.
For the working professional with moderate-to-significant symptoms who is functional enough to hold a job but not okay — the population the evening track was built for — iop treatment Orange County clinicians can offer something the data supports. Not a compromise on care. The care, scheduled around the life you are not willing to lose.
You are not gaming the system by choosing this format. You are matching the level of care to the level of need.
The Dual Diagnosis Reality Most Pages Skip
Anxiety, Depression, Trauma, and the Drink at 7 p.m.
Here is the part most program pages dance around.
You probably did not show up to your search bar with one tidy diagnosis. You showed up with a knot of things. The anxiety that has been louder for a year. The depression that flattens Sundays. The trauma you keep meaning to deal with. And the drink — or the edible, or the Xanax — at 7 p.m. that takes the edge off enough that you can sleep, parent, and do it again.
That is not two problems stacked on top of each other. That is one clinical picture. And it is the picture most working professionals actually walk in with.
If a program treats only the substance use, you will white-knuckle through abstinence while the anxiety that drove the drinking goes untouched, and the relapse math gets ugly fast. If a program treats only the mental health side and waves off the nightly wine, you will keep medicating the work you are doing in session and wonder why nothing is sticking.
The research on iop treatment Orange County programs and their peers nationally is clear on this point. A systematic review of intensive outpatient programs for co-occurring mental health and substance use disorders found that IOPs grounded in evidence-based therapies produce significant reductions in both substance use and psychiatric symptoms when the two are treated together, not in parallel silos 5.
What that means for you: a competent dual diagnosis IOP is not going to ask you to pick which thing is the “real” problem. It is going to treat the whole thing — the 7 p.m. drink and the 3 a.m. panic — as one system that needs one integrated plan.
How One IOP Week Integrates DBT, CBT, EMDR, and Medication
You know these acronyms. So let’s skip the textbook and talk about what they actually do inside one week of iop treatment Orange County clinicians can build for a co-occurring presentation.
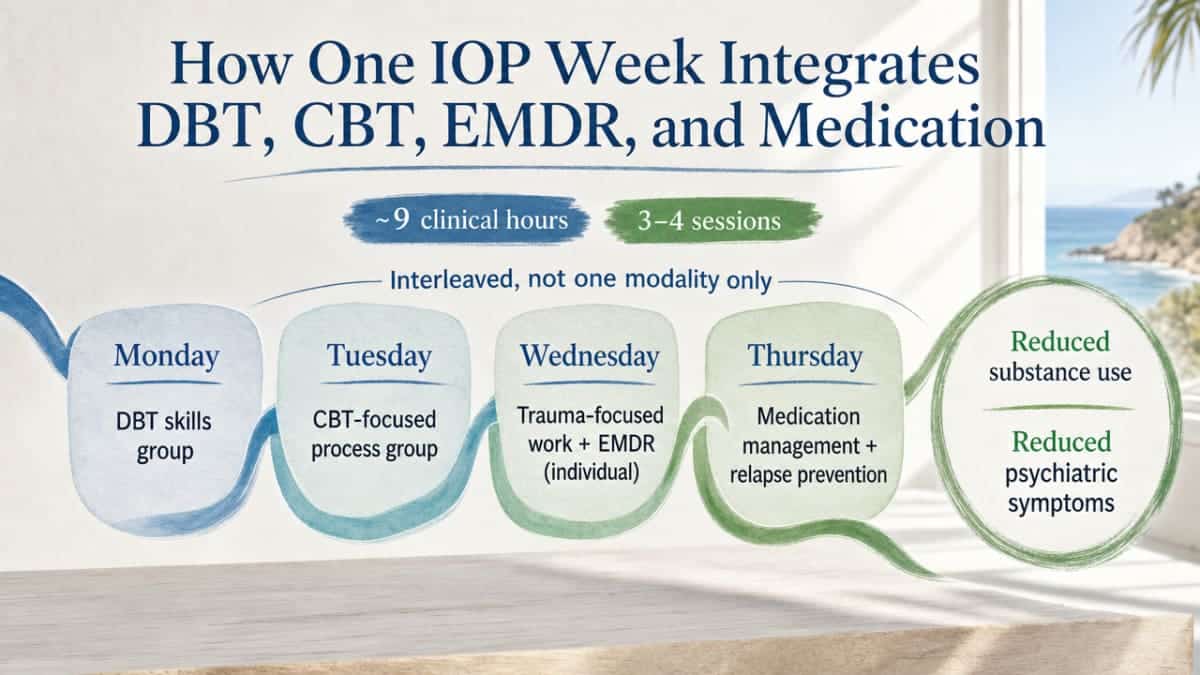
A typical evening IOP week is roughly nine clinical hours, spread across three or four sessions. Inside those nine hours, an integrated program does not pick one modality and stay there. It interleaves.
Monday is often DBT skills. Distress tolerance, emotion regulation, the specific tools you use at 7 p.m. when the urge to numb out hits. DBT is in the room because it gives you something to do with the feeling that is not a drink.
Tuesday tends to be a CBT-anchored process group. You walk through the thought patterns that drove your week — the catastrophizing before the Monday meeting, the rumination on the drive home — and you practice catching and reframing them in real time, with other people doing the same work.
Wednesday is where trauma-focused work, including EMDR, usually lives — typically in individual sessions, not group, because trauma processing is not safe to do in a circle of twelve strangers. EMDR is in your week because for a meaningful subset of professionals in dual diagnosis care, the trauma underneath is the engine the anxiety and the drinking are both attached to. You cannot skill-build your way out of an untreated trauma response forever.
Thursday often holds medication management with a psychiatric provider and a relapse prevention focus. If you are on an SSRI, a mood stabilizer, or in a medically supervised taper off benzodiazepines, this is where it gets monitored — not handed off to a primary care doctor who sees you twice a year.
Motivational interviewing threads through all of it. Not as a session on the schedule, but as the way clinicians talk to you when ambivalence shows up. And ambivalence will show up. Week three is usually when people decide this is too hard. Good clinicians expect that and work with it instead of arguing with it.
This is what integration means in iop treatment Orange County evening tracks: one week, multiple evidence-based modalities, one treatment plan that talks to itself. Pulling the modalities apart is what makes programs underperform.
You do not have to assemble this yourself. That is the whole point of the format.
Career, Confidentiality, and the Boss Conversation
Here is the fear you have probably not said out loud: if you do this, your career takes the hit.
You picture the calendar invite that someone asks about. The Wednesday you stop being available after 5:30. The HR meeting you do not want to have. You wonder if treatment ends up in a file somewhere, and whether the file ever follows you.
Let’s separate what is real from what is catastrophizing at 2 a.m.
What is real: an evening IOP track in iop treatment Orange County programs runs after most workdays end. You do not need to explain a 6 p.m. group the way you would explain a 1 p.m. one. If anyone asks, “I have a standing appointment” is a complete sentence. You owe coworkers a meeting status, not a diagnosis.
What is also real: your medical care is protected by federal privacy law, and substance use treatment records carry an additional layer of confidentiality under 42 CFR Part 2. Your employer does not get a call. Your manager does not get a chart note. If you use insurance, claims information is handled under HIPAA — not forwarded to HR.
The harder conversation is the one with yourself about whether to tell anyone at work at all. You do not have to. Plenty of professionals complete iop treatment Orange County evening tracks without naming it to a single colleague. Others find that telling one trusted person — a manager who has earned it, an HR partner who handles these requests routinely — actually lowers the daily load of hiding it.
If you do need formal accommodation, FMLA and ADA frameworks exist for exactly this. You can request intermittent leave for treatment without disclosing the underlying condition in detail. A clinician can write what is needed and nothing more.
Your job is not the price of getting better. For most working professionals choosing iop treatment Orange County clinicians design around evenings, the job is what gets protected — because you keep showing up to it, week after week, while the rest of you gets the care it has been waiting for.
Choosing a Program That Fits the 5 and 405
Geography is part of the clinical question here. It should not be, but it is.
If the program is in Newport and you live in Fullerton, a 5:30 p.m. start time means you are either leaving work at 4:15 or sitting on the 405 watching the clock burn. Three weeks of that and you are looking for reasons to skip. Engagement research on telehealth IOP makes this point directly: virtual and hybrid formats reduce the geographic and logistical barriers that quietly erode attendance for working adults 3.
So when you are comparing iop treatment Orange County programs, run the boring questions first.
- What time does group actually start, and what time does it end? A 6 p.m. start that runs to 9 is a different life than a 5 p.m. start that runs to 8. One lets you leave work on time. The other requires a conversation.
- Is the format hybrid by design, or hybrid as a backup? The distinction matters. A program that builds in some on-site sessions and some virtual ones is reflecting the evidence that mixed-modality outperforms exclusively remote care 4. A program that treats telehealth as the emergency option when you cannot make it in is a different product.
- Does the intake clinician actually ask about your week? Your commute, your kids’ pickup time, whether your manager has visibility into your calendar — those are clinical variables, not customer service ones. They predict whether you finish.
- How does the program handle dual diagnosis under one roof? If you have to bounce between a substance use track and a separate mental health provider who does not talk to your IOP team, you are doing the integration work yourself. That is not what integrated care means.
Pick the iop treatment Orange County program that makes the Tuesday after a hard Monday possible. Not the one with the prettiest website.
What Completion Actually Feels Like
You want to know what the other side of this looks like. Not the marketing version. The real one.
Completion of iop treatment Orange County clinicians design well does not feel like a finish line with a ribbon. It feels quieter than that. It feels like a Wednesday where you got through the 3 p.m. slump without the rumination spiral. It feels like the 7 p.m. urge showing up and you noticing it as a thought instead of a directive. It feels like sleeping through the night more often than not.
The satisfaction data tracks with that. In a peer-reviewed study of clients in a four-month integrated IOP for substance use disorders, mean satisfaction scores landed between 9.17 and 9.35 out of 10, with participants describing genuine personal growth across the program 10. That is a high bar, and it comes from people who did the whole thing.
Here is the honest part the brochures skip. That same body of work flags meaningful dropout rates 10. Some weeks are going to feel like too much. Week three is hard. Week seven is hard in a different way. The people who finish are not the ones who never wanted to quit. They are the ones who told their group they wanted to quit, and showed up the next Tuesday anyway.
Completion is not a personality. It is a practice of returning.
If you are reading this far, you are already doing the first part of the work. The next part is a phone call.
Frequently Asked Questions
Can I keep working full time while in IOP treatment Orange County programs offer?
Yes — that is exactly who evening tracks are built for. A standard IOP runs about nine clinical hours a week, typically across three or four sessions 1. Evening tracks load those hours into 6 to 9 p.m. blocks so your workday stays intact. Most clients in iop treatment Orange County evening formats keep working, parenting, and showing up Monday morning while doing the clinical work in the evenings.
How many hours per week does a standard evening IOP actually require?
Plan on roughly nine clinical hours, spread across three to four sessions per week, which is the dose the IOP evidence base consistently describes 1. An evening track keeps that same nine-hour weekly commitment but compresses it into 6 to 9 p.m. blocks. Add commute or login time, plus the homework and skills practice between sessions. It is real work — but it is engineered to coexist with a job.
Is virtual or hybrid IOP as effective as showing up in person?
The evidence is encouraging. One study of telehealth-delivered IOP for substance use disorders found that treatment retention and abstinence outcomes did not significantly differ from in-person care 6. A separate research brief noted that exclusively remote care can show slightly weaker results than mixed-modality delivery 4. That is why most credible iop treatment Orange County programs run hybrid by design — some on-site, some virtual — rather than picking one extreme.
Does my employer or my colleagues have to know I’m in treatment?
No. Your medical care is protected by federal privacy law, and substance use treatment records carry additional protection under 42 CFR Part 2. Your manager does not get a chart note. HR does not get a call. “I have a standing appointment” is a complete sentence for a 6 p.m. group. If you need formal accommodation, FMLA and ADA frameworks let a clinician document what is needed without disclosing your underlying diagnosis.
What if I’m dealing with both a mental health condition and drinking or substance use?
That is the picture most working professionals walk in with, and it has a name: co-occurring or dual diagnosis. A systematic review of IOPs for co-occurring mental health and substance use disorders found that programs using evidence-based therapies produce significant reductions in both substance use and psychiatric symptoms when the two are treated together 5. Look for iop treatment Orange County programs that integrate DBT, CBT, trauma work, and medication management under one plan.
How do I choose between PHP and IOP treatment Orange County clinicians recommend?
Acuity decides it, not preference. PHP runs around 20 or more clinical hours per week and fits people who need close daytime support but not 24-hour care. IOP runs about nine hours per week and fits people who are functional enough to keep working while doing the work 1. A good intake clinician will tell you directly which level matches your current symptoms, and step you down to IOP when PHP is no longer needed.
References
- Substance Abuse Intensive Outpatient Programs: Assessing the Evidence. https://pmc.ncbi.nlm.nih.gov/articles/PMC4152944/
- Substance Abuse Intensive Outpatient Programs: Assessing the Evidence (NCBI Bookshelf Overview). https://www.ncbi.nlm.nih.gov/books/NBK248088/
- Patient Engagement in Providing Telehealth SUD IOP Treatment. https://pmc.ncbi.nlm.nih.gov/articles/PMC11675410/
- The Effectiveness of Telehealth for Substance Use Disorder Treatment. https://practicetransformation.umn.edu/wp-content/uploads/2022/05/ResearchBrief_6_Effectiveness_Telehealth.pdf
- Effectiveness of intensive outpatient programs for co-occurring mental health and substance use disorders: A systematic review. https://pubmed.ncbi.nlm.nih.gov/33079678/
- Telehealth-delivered intensive outpatient treatment for substance use disorders: Outcomes and engagement. https://pubmed.ncbi.nlm.nih.gov/34751692/
- Intensive outpatient treatment for adolescents with depression and suicidality: Outcomes in a hospital-affiliated program. https://pubmed.ncbi.nlm.nih.gov/32745043/
- OC Community Health Improvement Plan 2024–2026. https://healthpolicy.ucla.edu/our-work/publications/oc-community-health-improvement-plan-2024-2026
- California Health Interview Survey (CHIS). https://healthpolicy.ucla.edu/our-work/california-health-interview-survey-chis
- Clients’ Experiences and Satisfaction with an Integrated Intensive Outpatient Treatment Program for Substance Use Disorders. https://pmc.ncbi.nlm.nih.gov/articles/PMC11898248/
- Behavioral Health Bureau | Orange County California. https://www.ocsheriff.gov/commands-divisions/patrol-operations-command/southwest-operations/behavioral-health-bureau



