Key Takeaways
- An intensive outpatient program in Orange County runs 9 to 19 hours per week under ASAM Level 2.1, with evening tracks built for adults who keep working, sleeping at home, and staying close to family 8.
- Orange County’s infrastructure has expanded around this need, with mental health and substance use named a top priority in the 2024-2026 Community Health Improvement Plan and Medi-Cal SUD benefits delivered through the Drug Medi-Cal Organized Delivery System 5, 6.
- Before enrolling, verify DHCS licensure, dual diagnosis capability under one integrated team, named modalities like DBT, CBT, EMDR, and motivational interviewing, evening scheduling specifics, in-network insurance status, and structured aftercare 7.
- Plan around a roughly 90-day intensive phase followed by lower-intensity step-down care, which research links to reduced substance use and better social functioning, with IOP outcomes comparable to inpatient for many people 9, 2.
What clinical intensity actually means when you’re still working full-time
You’ve probably been thinking about this for a while. The 6 a.m. anxiety. The drinking that started as decompression and became something else. The trauma response that keeps showing up in meetings. And somewhere in the middle of all that, the quiet question: do I need real treatment, or can I keep handling this on my own?
An intensive outpatient program orange county sits in a specific spot on the clinical map. It’s not weekly talk therapy, where you see someone for 50 minutes and try to apply the work between sessions. It’s not residential care, where you leave your life for 30 or 60 days. It’s the level designed for adults who need more than once-a-week support but who can still sleep at home, keep their job, and stay close to their family.
Clinically, that translates to multiple hours of structured care across several days per week — group work, individual sessions, and psychiatric oversight when needed. The intensity is real. So is the flexibility. Evening tracks exist precisely because the people who need this level of care are often the same people running teams, managing households, and showing up to a Tuesday standup at 9 a.m.
The rest of this guide walks you through what that actually looks like — hours, modalities, licensure, insurance, outcomes — so you can evaluate an intensive outpatient program orange county on clinical terms, not marketing terms.
How an intensive outpatient program orange county fits between weekly therapy and residential care
The 9-19 hour weekly range and why it matters for your calendar
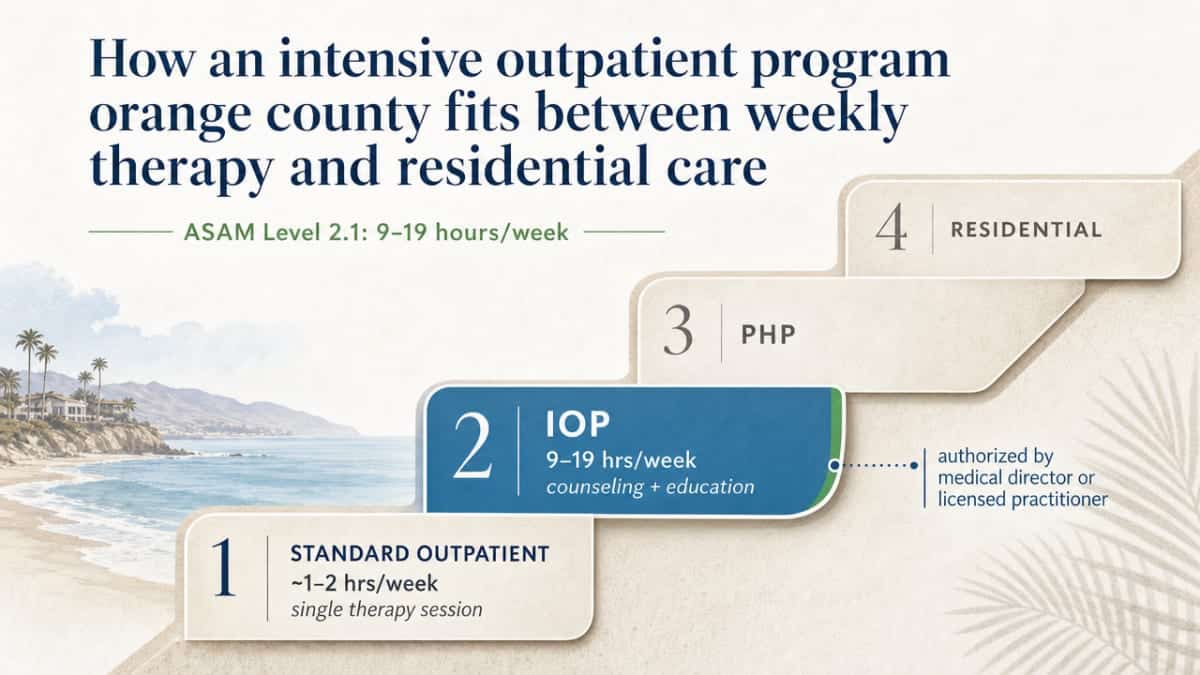
Here’s the number that actually shapes your week: California’s Department of Health Care Services defines adult intensive outpatient treatment at ASAM Level 2.1 as a minimum of 9 and a maximum of 19 hours per week, primarily counseling and education, authorized by a medical director or licensed practitioner 8. That’s the regulatory spine of any intensive outpatient program orange county provider, whether you’re paying through commercial insurance or Medi-Cal.
Think of the continuum as a ladder. At the bottom rung sits standard outpatient therapy — roughly one or two hours a week, usually a single session with a therapist. One rung up is the intensive outpatient program orange county level: 9 to 19 hours weekly, spread across three to five days, blending group work with individual sessions 8. Above that is partial hospitalization, which typically runs 20 or more hours a week and looks closer to a structured day program. At the top is residential or inpatient care — 24/7 supervision, life paused.
For a working professional, the 9-19 hour range is the difference-maker. A common evening configuration looks like three nights a week, three hours per night — nine hours, the floor of the range. A more clinically intensive track might add a fourth evening or a Saturday group, pushing you closer to the upper end. Either way, the hours land outside your standard workday. You finish at five, drive twenty minutes, and you’re in group by six. You’re home by nine-thirty.
That arithmetic matters because it tells you, before you ever call admissions, what kind of footprint treatment will leave on your calendar.
Why this level of care exists, and who it’s designed for
This level of care exists because the gap between weekly therapy and residential treatment is huge — and most people who need real help fall somewhere in the middle. Medicare describes it plainly: intensive outpatient programs sit between traditional once-weekly therapy and inpatient hospital care, offering structured services for mental health conditions including substance use disorders 4. SAMHSA’s clinical guidance frames intensive outpatient treatment as part of a continuum that has deliberately expanded to serve a wider variety of clients, with individualized, evidence-based approaches at its core 3.
So who is this designed for? You, if any of this sounds familiar. You’re holding down a job in Irvine, Newport Beach, or Anaheim, but the anxiety has gotten loud enough that you’re losing sleep three nights a week. You’ve tried weekly therapy and it helps, but it’s not enough to interrupt the pattern. You’re functional — meetings happen, deadlines get met — but the cost of staying functional is rising. Maybe alcohol or a prescription is doing more of the work than it used to.
An intensive outpatient program orange county track is built for the person who needs clinical intensity without needing to leave their life. You’re not in crisis. You don’t need a hospital bed. You need structure, evidence-based therapy, and enough hours per week that real change becomes possible.
Inside an evening IOP track: structure, modalities, and what a week looks like
Group therapy, individual sessions, and psychiatric care under one roof
A well-built evening track isn’t just group after group after group. It’s a layered week that blends three distinct clinical components, and understanding what each one does will help you ask sharper questions when you call admissions.
The bulk of your hours in an intensive outpatient program orange county happen in group therapy. That’s by design. Groups give you practice — not just talking about what’s happening in your life, but working through it alongside other adults who get it. A Monday evening process group might run ninety minutes. A Wednesday skills group might focus on emotion regulation or relapse prevention education. Thursday could be a trauma-focused group or a family dynamics group. The content rotates so the week builds on itself instead of repeating.
Individual therapy sits underneath the group work. You’ll typically meet one-on-one with a primary therapist on a regular cadence — often weekly — to translate what’s surfacing in group into your specific situation. This is where the work gets personal: your relationship with your spouse, the pattern that keeps showing up at work, the specific trauma you’re not ready to discuss in front of seven other people.
Psychiatric care is the third leg. If medication is part of your treatment, or if it might become part of it, a psychiatrist or psychiatric nurse practitioner oversees that piece — evaluation, prescribing, adjustments, and coordination with the rest of the team. SAMHSA’s clinical guidance is clear that high-quality intensive outpatient treatment is individualized and evidence-based across all of these components, not bolted together from disconnected services 3.
The evidence-based modalities to look for: DBT, CBT, EMDR, motivational interviewing
Modalities are the actual therapeutic methods being used in those groups and individual sessions. This is where program quality separates fast. When you’re evaluating an intensive outpatient program orange county, ask which modalities are core to the curriculum and which clinicians are trained to deliver them.
Dialectical Behavior Therapy, or DBT, was originally developed for borderline personality disorder but has become a workhorse for emotion regulation, distress tolerance, and interpersonal effectiveness across many conditions. If you’ve ever felt like your emotional responses are out of proportion to the trigger — or that you swing between numb and overwhelmed without much in between — DBT skills give you concrete tools for the in-between.
Cognitive Behavioral Therapy (CBT) is the most-studied modality for anxiety and depression. It targets the loop between thoughts, feelings, and behaviors. For a working professional whose anxiety has wired itself into specific situations — Sunday nights, performance reviews, social events with drinking — CBT does the unglamorous, effective work of interrupting that loop.
EMDR (Eye Movement Desensitization and Reprocessing) is the modality you want available if trauma is part of the picture. It’s specifically designed to reprocess traumatic memories so they stop hijacking the present.
Motivational interviewing is less a single technique and more a conversational stance. It helps you work through ambivalence — the part of you that knows something has to change and the part that isn’t sure you’re ready. SAMHSA’s clinical protocol describes high-quality intensive outpatient care as deliberately drawing on these kinds of evidence-based approaches, individualized to the person in front of the clinician rather than forced through a single template 3.
If a program can’t name its modalities, or names them only vaguely, keep asking.
Dual diagnosis: when anxiety, depression, or trauma travel with substance use
For a lot of professionals reaching this point, the question isn’t anxiety or substance use. It’s both, tangled together. The anxiety started first, the drinking became how you managed it, and now the drinking is making the anxiety worse. Or trauma you never fully processed is driving both the depression and the pattern you can’t quite break.
That’s dual diagnosis, and treating both conditions at the same time — under one clinical team, in one coordinated plan — is the standard of care. Splitting them apart, sending you to one provider for the mental health piece and another for the substance use piece, tends to leave the most important part untouched: the way they feed each other.
SAMHSA’s clinical guidance specifically calls out the value of individualized, evidence-based intensive outpatient care that can serve a wider variety of clients — including those whose presentations don’t fit neatly into a single diagnostic box 3. When you’re evaluating an intensive outpatient program orange county, ask directly whether the program treats co-occurring mental health and substance use disorders together, who oversees the integration, and how psychiatric care, individual therapy, and group work coordinate around your specific combination.
Vetting a program in Orange County: a clinical checklist, not a brochure tour
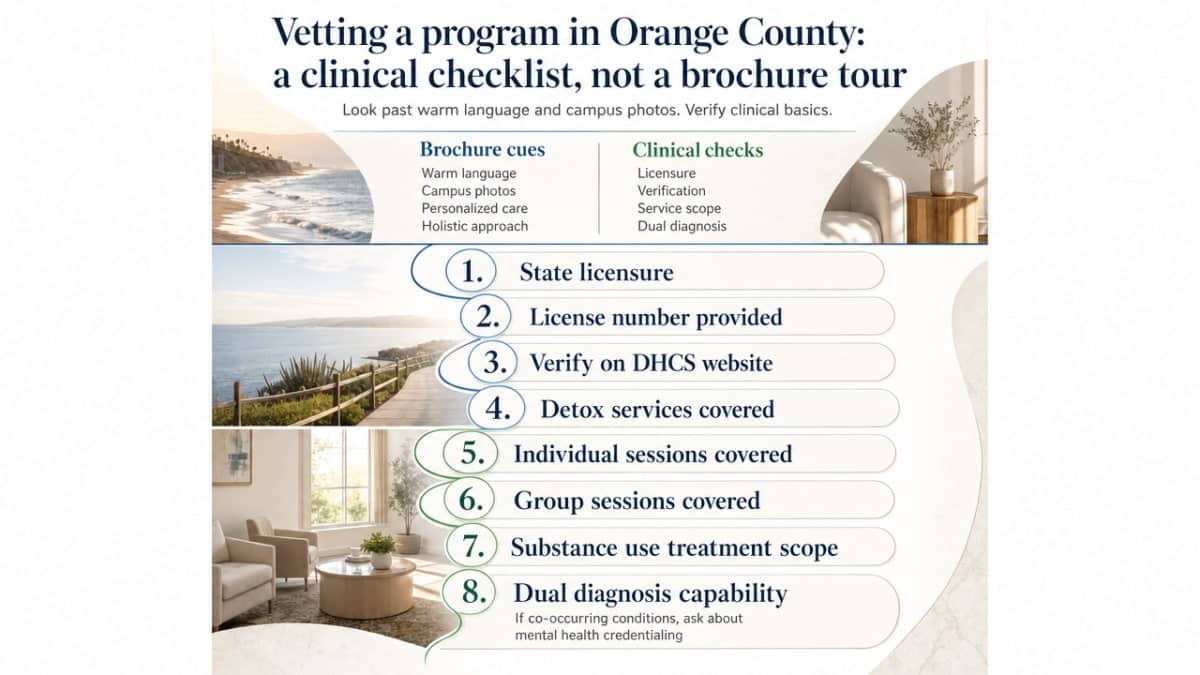
When you call admissions at an intensive outpatient program orange county provider, you’re going to hear warm language. Beautiful campus photos. Phrases like “personalized care” and “holistic approach.” None of that tells you whether the program is clinically sound. These are the things that do.
State licensure. California requires programs to be licensed or certified by the Department of Health Care Services when they provide detoxification, individual sessions, group sessions, or other services to treat substance use disorders 7. Ask for the license number. A legitimate program will give it to you without hesitation, and you can verify it directly on the DHCS website. If a program treats co-occurring conditions, ask how it’s also credentialed for mental health care.
Dual diagnosis capability. If anxiety, depression, trauma, or another mental health condition is part of your picture alongside substance use, ask specifically whether one integrated team treats both — or whether the program coordinates with an outside provider for half of it. The answer changes your weekly experience.
Named modalities. The program should be able to tell you, by name, which evidence-based approaches it uses — DBT, CBT, EMDR, motivational interviewing — and which clinicians are trained in each. SAMHSA’s clinical guidance is built around individualized, evidence-based care, not a one-size template 3.
Clinical leadership. Ask who the chief clinical officer or clinical director is, what their license is (LMFT, LCSW, psychologist, psychiatrist), and how often they’re actually on-site. Programs with absent clinical leadership tend to drift.
In-network status. Ask which commercial insurers the program is in-network with — Blue Shield, Cigna, Anthem, Aetna, and others common in Orange County. In-network status changes what you’ll pay out of pocket and how the authorization process works.
Evening scheduling. If you’re working full-time, confirm the evening track exists, which nights it runs, and what the start and end times actually are. “Flexible scheduling” without specifics often means a daytime program with a few exceptions.
Structured aftercare. What happens at week twelve? A real program has a step-down plan — lower-intensity outpatient groups, alumni support, continued individual therapy — built into the discharge process, not improvised at the end.
Family involvement. Ask whether family therapy or family education sessions are part of the curriculum. The people closest to you are part of how recovery holds.
Write these down before you call. An intensive outpatient program orange county provider that answers each one cleanly is showing you exactly the kind of clinical depth you’re looking for.
How insurance and coverage actually work for outpatient mental health care
Commercial insurance, Medi-Cal, and Medicare pathways
Coverage for an intensive outpatient program orange county track usually runs through one of three doors, and which one applies to you shapes the conversation you’ll have with admissions.
If you’re a working professional with commercial insurance through your employer — Blue Shield of California, Cigna, Anthem, Aetna, or similar — intensive outpatient is typically a covered behavioral health benefit. The mechanics involve a medical necessity review, usually authorized in blocks of sessions, with the program submitting clinical documentation on your behalf. In-network status changes your out-of-pocket exposure significantly, so confirming the program contracts directly with your carrier is one of the first questions worth asking.
If you’re on Medi-Cal, intensive outpatient treatment has been a covered benefit statewide since California expanded SUD services under the Affordable Care Act 1. Access in Orange County runs through the Drug Medi-Cal Organized Delivery System, which California’s Department of Health Care Services describes as the structured framework for delivering substance use disorder treatment services across counties 6. That system includes a statewide non-emergency SUD treatment referral line you can call to be routed to participating providers 6.
If you’re helping a parent or older family member, Medicare Part B covers intensive outpatient services for mental health conditions, including substance use disorders, as a level of care that sits between weekly therapy and inpatient hospitalization 4. Different door, same continuum.
Questions to ask before your first session
Before you sign anything, get clear answers to a short list of questions. Is the program in-network with your specific insurance plan, not just the carrier name? What’s the authorization process — does the program handle the medical necessity submission, or are you the one chasing approvals? How many sessions are typically authorized at a time, and what triggers a continued-stay review?
Ask about the financial counselor on staff. A serious intensive outpatient program orange county provider has someone whose entire job is walking you through your benefits in plain language before treatment starts. Ask for a written estimate of your responsibility for the full episode of care, not just the first week.
If you’re on Medi-Cal, ask whether the program participates in the county’s Drug Medi-Cal network 6. If you’re on Medicare, confirm the program bills Part B for intensive outpatient services 4. The right answers come quickly. Hesitation is information.
How long IOP lasts and what realistic outcomes look like
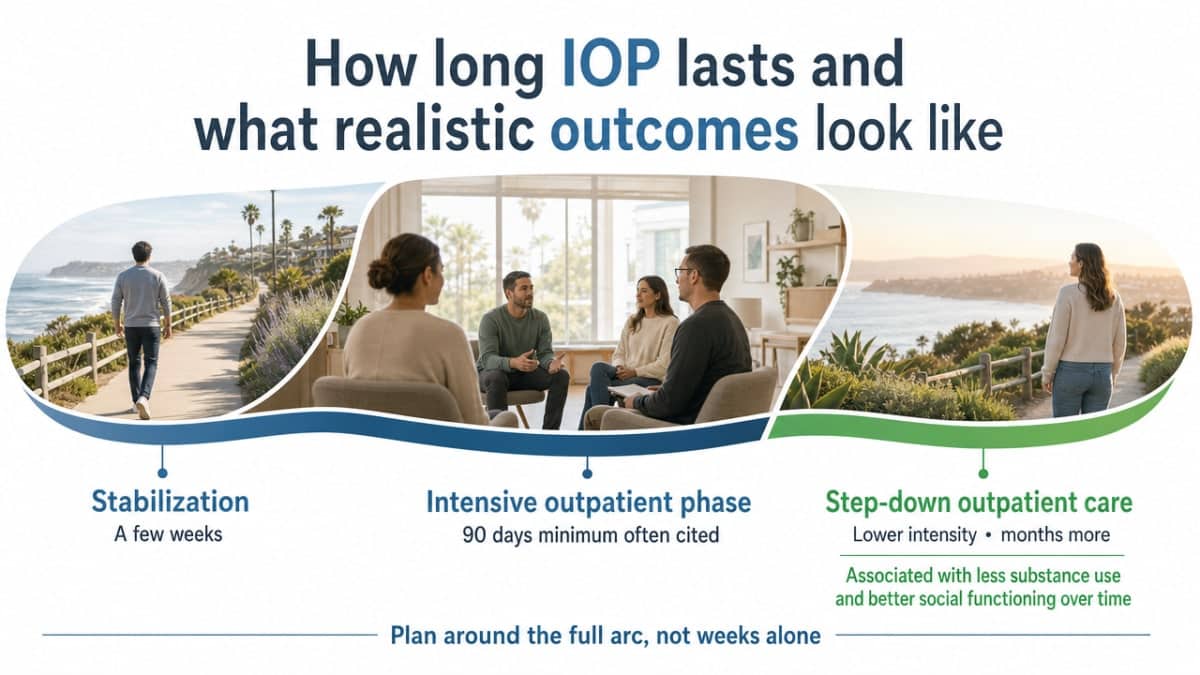
You’re going to want a timeline. Most people do. The honest answer is that an intensive outpatient program orange county track isn’t measured in weeks alone — it’s measured in the arc of stabilization, structured intensity, and what comes after.
SAMHSA’s clinical guidance puts a marker in the ground: the recommended minimum duration of the intensive outpatient phase is often cited as 90 days, and extended lower-intensity outpatient care after that phase is associated with less substance use and better social functioning over time 9. That’s the arc to plan around. A few weeks of stabilization as you settle into the rhythm, roughly three months at full IOP intensity, then a step down into less frequent groups and continued individual therapy that can extend for months more.
Ninety days sounds like a long time when you’re staring at your calendar. It’s shorter when you think about what it’s actually doing. You’re not just reducing symptoms during those weeks — you’re building skills, untangling the patterns underneath, and practicing them in real time while you go to work, eat dinner with your family, and handle the ordinary friction of a Tuesday. The lower-intensity care that follows is what helps those skills hold.
What do realistic outcomes look like? A systematic review in Psychiatric Services found that intensive outpatient programs can be as effective as inpatient treatment for many individuals with substance use disorders when comparable services are delivered 2. That’s a meaningful finding, and it deserves its scope: the review looked at multiple studies of SUD IOPs, not every condition treated in outpatient care, and outcomes vary with program quality and individual fit. Still, the headline holds — you don’t have to leave your life to get care that works.
Real outcomes also look like things that don’t show up in research papers. Sleeping through the night again. Sitting in a meeting without your heart racing. Saying no to a second drink without it taking everything you have. Being present at your kid’s soccer game instead of mentally rehearsing tomorrow’s email. Those are the metrics that matter when you’re the one living it.
The Orange County context: why local infrastructure has expanded around mental health
You’re not making this decision in a vacuum. Orange County’s behavioral health system has been expanding around exactly the kind of need you’re sitting with, and that shift didn’t happen by accident.
The Orange County Community Health Improvement Plan for 2024-2026 names six priority areas its stakeholders identified, and mental health and substance use sit at the top of that list — alongside housing, care navigation, and economic well-being 5. That’s not a vague endorsement. It’s a planning document that shapes where funding, partnerships, and provider capacity get directed across the county over multiple years.
The financing infrastructure has moved in the same direction. California expanded Medi-Cal substance use disorder benefits to include intensive outpatient treatment as a covered service 1, and the Drug Medi-Cal Organized Delivery System gave counties a structured framework for delivering that care, including a statewide non-emergency referral line 6. Commercial carriers operating in Orange County have followed the same trajectory, contracting with a wider network of outpatient mental health providers than existed a decade ago.
What that means for you: when you start calling an intensive outpatient program orange county provider this week, you’re walking into a system that has been deliberately built up to meet you. The infrastructure is here because people like you needed it to be.
Making the call: what to do this week
You’ve done the hard part already. You’ve read this far, which means you’ve stopped circling the decision and started shaping it. That counts.
Here’s what a useful next seven days looks like. Pull your insurance card and find the behavioral health number on the back. Write down three or four questions from the vetting list — licensure, dual diagnosis capability, named modalities, evening track specifics — and keep them next to your phone. Then call two or three providers offering an intensive outpatient program orange county track. Listen for how they answer. A program that can speak clearly about ASAM Level 2.1 hours, integrated care, and aftercare structure is showing you something real.
You don’t have to have it all figured out before you dial. Admissions teams expect questions. Ask for a clinical assessment — that’s the conversation where fit gets determined, not the website. If you’re weighing an evening intensive outpatient program orange county option through a provider like 449 Recovery in Mission Viejo, the assessment is where you’ll learn whether the schedule and clinical approach actually match your week. One call this week. That’s the step.
Frequently Asked Questions
How many hours per week will I actually spend in an intensive outpatient program orange county?
For adults, California’s Department of Health Care Services sets the range at a minimum of 9 and a maximum of 19 hours per week, primarily counseling and education 8. A common evening schedule lands at the floor — three nights a week, three hours per night. More clinically intensive tracks add a fourth evening or weekend group.
Can I keep working full-time while attending an intensive outpatient program orange county?
Yes — that’s exactly what the evening track is built for. Sessions typically run after standard work hours, so you can finish your day, drive to the program, and be home by mid-evening. Confirm specific start and end times with admissions, and ask whether the program has experience supporting working professionals through medical leave conversations if your schedule needs short-term adjustment.
How do I know if a program is properly licensed in California?
The Department of Health Care Services requires licensure when programs provide detoxification, individual sessions, group sessions, or other services to treat substance use disorders 7. Ask the program for its license number directly. A legitimate provider will share it without hesitation, and you can verify it on the DHCS website before your first session.
What if I’m dealing with anxiety or depression along with substance use?
That combination is common, and treating both conditions together under one clinical team is the standard of care. SAMHSA’s clinical guidance emphasizes individualized, evidence-based intensive outpatient care designed to serve clients whose presentations don’t fit a single diagnostic box 3. Ask any intensive outpatient program orange county provider whether one integrated team handles both — or whether they refer half out.
How long does IOP typically last before stepping down to a lower level of care?
SAMHSA’s clinical guidance cites a recommended minimum duration of about 90 days for the intensive outpatient phase, with extended lower-intensity outpatient care afterward associated with less substance use and better social functioning over time 9. Expect roughly three months at full intensity, then a step-down into less frequent groups and continued individual therapy that can extend for months.
Will my commercial insurance, Medi-Cal, or Medicare cover intensive outpatient treatment?
Usually yes, through three different doors. Commercial plans typically cover IOP as a behavioral health benefit with medical necessity review. Medi-Cal includes intensive outpatient treatment as a covered substance use benefit statewide 1, delivered through the Drug Medi-Cal Organized Delivery System 6. Medicare Part B covers IOP services for mental health conditions, including substance use disorders 4.
References
- Expanded Benefits – DHCS – CA.gov. https://www.dhcs.ca.gov/provgovpart/Pages/ExpandedBenefits.aspx
- Substance Abuse Intensive Outpatient Programs: Assessing the Evidence. https://pmc.ncbi.nlm.nih.gov/articles/PMC4152944/
- TIP 47: Substance Abuse: Clinical Issues in Intensive Outpatient Treatment. https://www.samhsa.gov/resource/ebp/tip-47-substance-abuse-clinical-issues-intensive-outpatient-treatment
- Mental health care (intensive outpatient program services) – Medicare. https://www.medicare.gov/coverage/mental-health-care-intensive-outpatient-program-services
- OC Community Health Improvement Plan 2024-2026 (UCLA Health Policy). https://healthpolicy.ucla.edu/our-work/publications/oc-community-health-improvement-plan-2024-2026
- Drug Medi-Cal Organized Delivery System – DHCS – CA.gov. https://www.dhcs.ca.gov/provgovpart/Pages/Drug-Medi-Cal-Organized-Delivery-System.aspx
- Licensing and Certification Facility Licensing – DHCS. https://www.dhcs.ca.gov/provgovpart/Pages/Licensing-and-Certification-Facility-Licensing.aspx
- Intensive Outpatient Treatment and the Drug Medi-Cal Organized Delivery System (FAQ). https://www.dhcs.ca.gov/provgovpart/Documents/DMC-ODS_Waiver/DMC_ODS_IOT_FAQ_06.18.pdf
- Chapter 3. Intensive Outpatient Treatment and the Continuum of Care. https://www.ncbi.nlm.nih.gov/books/NBK64088/



