Key Takeaways
- Master the Cognitive Triangle: Understand how cognitive behavioral therapy for anxiety disrupts the reinforcing loop between thoughts, feelings, and behaviors to reduce symptom severity.
- Integrate Dual Diagnosis Care: Utilize transdiagnostic protocols to treat anxiety and substance use disorders simultaneously, preventing fragmented care and improving outcomes.
- Leverage Digital Tools: Overcome access barriers by incorporating smartphone-based CBT and blended care models, which show remission rates comparable to in-person treatment.
- Commit to Practice: Recognize that consistent engagement with tools like exposure hierarchies and thought records is essential for rewiring anxious patterns.
How Cognitive Behavioral Therapy for Anxiety Rewires Thought Patterns
The Cognitive Triangle Framework
The Cognitive Triangle is a foundational tool in cognitive behavioral therapy for anxiety. This framework helps you visualize how thoughts, feelings, and behaviors interact in a reinforcing loop. When anxious thoughts take hold, they often spark strong emotional responses, which then drive avoidance or safety behaviors. Over time, these patterns can become automatic and deeply embedded.
“I can’t handle this.” — A common automatic thought that triggers dread and avoidance behaviors.
To use the Cognitive Triangle in practice, start by mapping out a recent anxiety episode. By breaking down these moments, you can spot unhelpful thinking traps—like catastrophizing or overgeneralization—and begin to test their accuracy. This process is essential for disrupting the anxiety cycle and building more adaptive responses9. Ask yourself the following questions to guide this reflection:
- What were my automatic thoughts?
- How did I feel, both emotionally and physically?
- What did I do next (behavior)?
Applying the Cognitive Triangle requires a time investment—typically 10-15 minutes per reflection exercise, either independently or during a session. All you need is paper, a pen, and openness to honest self-inquiry. This approach works best when you’re ready to challenge old patterns and celebrate incremental change. Yes, it can feel uncomfortable at first, and that’s completely normal. Progress comes from consistent practice and noticing even the smallest shifts in thinking.
Evidence Base Across Anxiety Disorders
When weighing the evidence for cognitive behavioral therapy for anxiety, it’s clear you’re working with one of the most thoroughly researched interventions in mental health. Meta-analyses consistently show strong outcomes across a spectrum of anxiety disorders. Response rates for CBT generally range from 50% to 80% in conditions like panic disorder, generalized anxiety disorder (GAD), social anxiety, obsessive-compulsive disorder (OCD), and post-traumatic stress disorder (PTSD)6.

| Condition | Effect Size / Outcome | Clinical Note |
|---|---|---|
| Panic Disorder | Small effect (g=0.35) | Variable response; may require medication adjunct. |
| OCD | Large effect (g=1.37) | Highly responsive to exposure-based protocols1. |
| GAD (Digital CBT) | 71% Remission Rate | Comparable to or better than psychoeducation alone9. |
Digital and blended models of CBT have expanded access and demonstrated remission rates as high as 71% for adults with GAD using smartphone-based programs. This solution fits busy professionals or those in rural areas who may struggle with scheduling or transportation. If you’re managing dual diagnosis or complex presentations, research supports transdiagnostic CBT protocols that can flexibly target anxiety alongside other co-occurring symptoms7.
Yes, it’s challenging to see clients drop out—exposure-based protocols for PTSD average a 21% dropout rate, higher than placebo conditions3. But even small reductions in avoidance or distress are meaningful wins. Every incremental shift matters.
Core Therapeutic Components of Cognitive Behavioral Therapy for Anxiety
Cognitive Restructuring Techniques
Cognitive restructuring is a practical, hands-on technique at the heart of cognitive behavioral therapy for anxiety. At its core, cognitive restructuring means helping clients recognize and challenge unhelpful thinking patterns—like catastrophizing, black-and-white thinking, or personalizing. Use the following checklist during sessions or self-reflection to guide the process:
- Identify the Trigger: Pinpoint the specific event and the associated anxious thought.
- Capture the Thought: Write down the automatic thought exactly as it appears.
- Examine the Evidence: List facts that support the thought and facts that contradict it.
- Generate Alternatives: Create a more balanced or realistic perspective based on the evidence.
- Re-evaluate: Notice any shifts in emotional response or behavior after the exercise.
For example, when a client voices, “I’ll embarrass myself at the meeting,” walk with them through the evidence: What’s the proof? How likely is this outcome? What happened before in similar situations? This supportive questioning helps them develop more flexible, less distressing perspectives. In practice, most clinicians spend 10-20 minutes per session guiding a restructuring exercise. You’ll need a worksheet, pen, and a willingness to sit with discomfort as beliefs are tested.
This approach is ideal for clients who ruminate or struggle with persistent worry—especially if they feel stuck in loops of negative prediction or self-criticism. Every shift toward a more adaptive thought is a genuine win, no matter how small. Research consistently finds that cognitive restructuring reduces anxiety symptoms and increases treatment engagement, especially when paired with behavioral interventions like exposure6.
Exposure Therapy Protocols and Mechanisms
Exposure therapy is a cornerstone technique within cognitive behavioral therapy for anxiety, designed to help clients systematically confront feared situations, memories, or sensations. Exposure therapy works by promoting habituation—a reduction in anxiety through repeated, safe contact with feared stimuli. This process also fosters extinction, meaning old fear associations weaken when the expected negative outcome doesn’t occur.

- List triggers from least to most anxiety-provoking.
- Assign each an anxiety rating (0-10 scale).
- Begin exposures with lower-rated items, using brief, repeated practice.
- Gradually progress to more challenging steps as confidence increases.
- Track anxiety levels before, during, and after each exposure.
Over time, clients gain emotional processing skills and increased self-efficacy, making anxiety feel less overwhelming3. In clinical settings, a single exposure session might last 30-60 minutes. Preparation, debriefing, and support between sessions are vital, especially when working with trauma histories or severe avoidance. You’ll need a worksheet, timer, and sometimes creative tools like audio recordings or virtual reality for specific phobias.
Prioritize this when clients are stuck in avoidance cycles or when other strategies haven’t yielded significant anxiety reductions. Exposure therapy dropout rates are higher than some other interventions—averaging 21% in PTSD trials—but each completed exposure is a step toward reclaiming daily functioning3. Yes, it’s tough work, and that’s okay. Small gains, like tolerating mild discomfort, deserve recognition.
Treating Co-Occurring Anxiety and Substance Use
Transdiagnostic Approaches for Dual Diagnosis
When treating co-occurring anxiety and substance use, transdiagnostic approaches offer you a flexible, evidence-based pathway. A transdiagnostic approach means you use a single cognitive behavioral therapy for anxiety protocol that targets the shared underlying processes fueling both conditions—like avoidance, rigid thinking, or emotional dysregulation—instead of addressing each diagnosis separately. This can streamline care and reduce the risk of fragmented interventions.
Use this quick assessment tool to guide your clinical decision-making:
- Identify Overlap: Look for shared symptoms like avoidance, negative thinking, or impulsivity.
- Screen for Triggers: Find patterns that cut across both anxiety and substance use.
- Determine Readiness: Assess motivation, stability, and support for integrated CBT.
- Map Priorities: Decide which symptoms are most impairing right now.
This strategy suits you if your caseload includes clients with complex presentations, limited resources, or frequent diagnostic overlap. Research highlights that transdiagnostic CBT protocols, like the Unified Protocol, can effectively address anxiety and substance use simultaneously, improving engagement and outcomes without the need for multiple, siloed treatments7. You’ll typically invest 12-20 weeks, with each session lasting 45-60 minutes, and require training in transdiagnostic CBT models along with strong case formulation skills.
Sequencing and Integration Considerations
Sequencing and integration are critical when applying cognitive behavioral therapy for anxiety in cases where substance use is also present. Opt for parallel treatment models if your client is stable enough to address both anxiety and substance use together, as this supports skill generalization and reduces the risk of one disorder undermining gains in the other. Here is a practical planning tool to help you navigate this process:
- Assess acute safety risks (withdrawal, suicidality, medical instability).
- Stabilize substance use and address immediate crises first if necessary.
- Evaluate readiness for anxiety-focused work (motivation, cognitive clarity).
- Decide if parallel, sequential, or fully integrated CBT delivery is most appropriate.
- Coordinate with other providers and align goals across the care team.
Click to Compare: Sequential vs. Integrated Models
Sequential Approaches: Treating substance use first, then anxiety. This makes sense when acute intoxication or withdrawal symptoms would interfere with therapy engagement.
Integrated CBT Models: Blending anxiety and substance use interventions within each session. This has growing support and can improve outcomes for dual diagnosis clients7.
This approach works best when you have access to multidisciplinary collaboration and regular case review. Typically, sequencing and integration planning requires 1-2 hours for initial assessment and ongoing coordination at each treatment phase. Yes, these decisions can be tough and the path isn’t always linear, but each step toward a more unified plan brings you—and your clients—closer to meaningful progress.
Digital Delivery and Implementation Models
Blended Care and Smartphone-Based CBT
Blended care—where in-person and digital sessions are combined—has become a practical and flexible option for delivering cognitive behavioral therapy for anxiety. Smartphone-based CBT programs, in particular, empower you to extend therapy beyond the office, allowing clients to complete mood tracking, skill practice, or thought records at any time. A straightforward tool for blended care includes setting up digital check-ins: schedule weekly app-based homework, monitor engagement, and use session time to review progress and troubleshoot barriers.
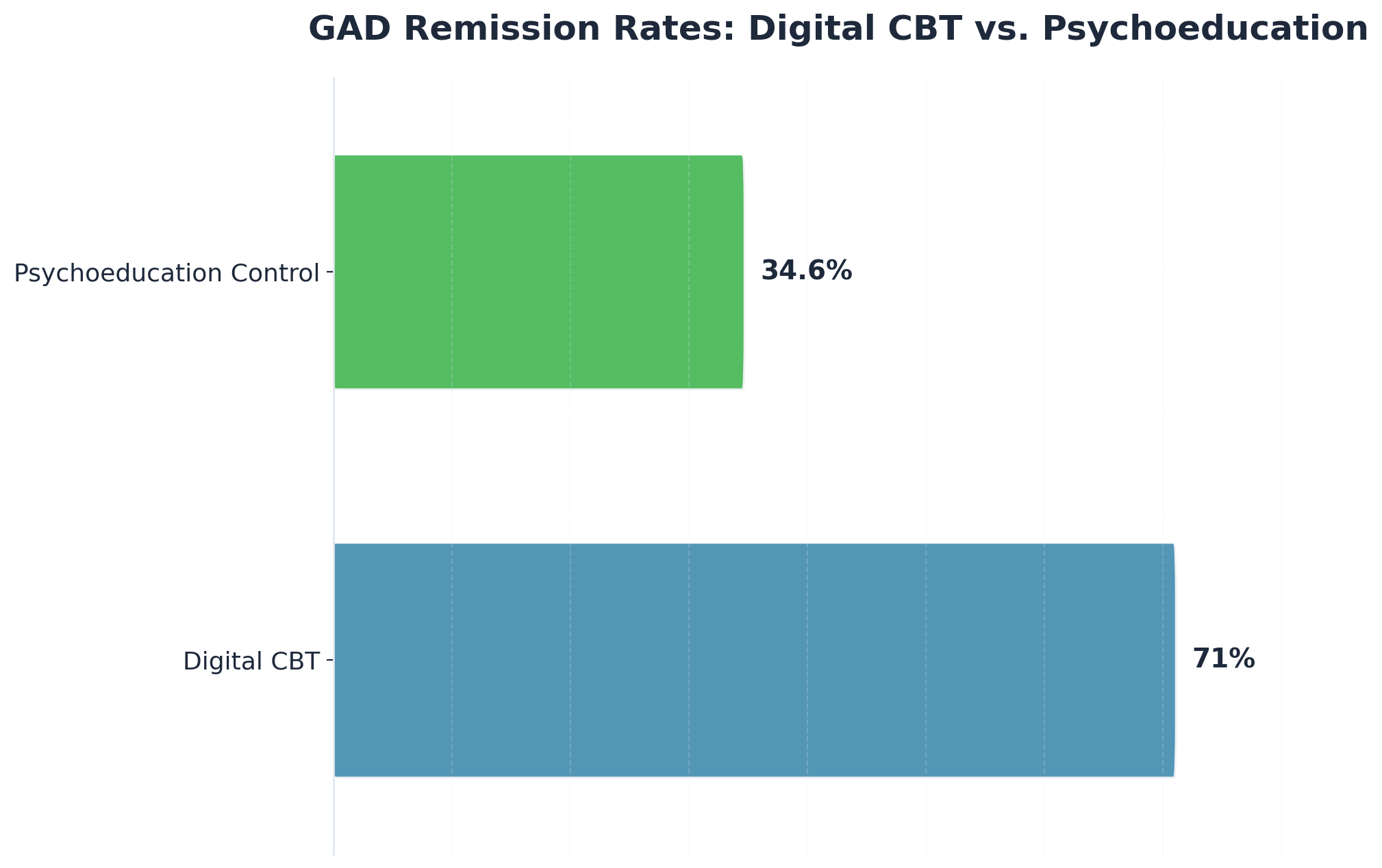
This approach is ideal when your clients are juggling work, family, or fluctuating motivation. Research demonstrates that 71% of adults with generalized anxiety disorder (GAD) achieved remission with smartphone-based CBT, compared to 34.6% who received psychoeducation alone9. You’ll typically invest 10-15 minutes onboarding clients to the app or platform, with ongoing support as needed. Resource requirements include a HIPAA-compliant app, a reliable internet connection, and periodic monitoring of digital data.
If you’re working with dual diagnosis, blended models can increase accessibility and reinforce skills between sessions—especially important for those with transportation or scheduling challenges. Every digital check-in or completed exercise is a small win worth celebrating.
Barriers in Community Mental Health Settings
Barriers to implementing cognitive behavioral therapy for anxiety through digital models in community mental health settings often stem from practical and systemic challenges. Lack of clinician training is a top barrier—many organizations struggle to provide ongoing education for digital CBT tools. Use this quick assessment to pinpoint the most common obstacles:
- Does your team have sufficient digital literacy and training?
- Are there reliable devices and internet access for clients and staff?
- Is there organizational buy-in for blended or smartphone-based care?
- Are privacy and HIPAA compliance protocols clear and supported?
Limited funding for technology and infrastructure can leave both providers and clients without the resources needed to sustain virtual care. Organizational resistance may arise from concerns that cognitive behavioral therapy for anxiety is too rigid or not well suited for clients with complex, co-occurring diagnoses—though research shows digital CBT can be effective across populations6. This path makes sense when your clinic has invested in staff training, reliable technology, and clear protocols for digital care. Yes, adapting to new modalities is tough, but every effort to break down these barriers increases access to evidence-based anxiety treatment.
Frequently Asked Questions
What should I expect during the first few weeks of cognitive behavioral therapy for anxiety?
During the first few weeks of cognitive behavioral therapy for anxiety, you can expect to focus on building trust with your therapist, learning about the CBT model, and identifying your unique anxiety triggers. Early sessions often involve tracking your thoughts, feelings, and behaviors in real time, which may feel unfamiliar or even uncomfortable—this is completely normal. You’ll likely be introduced to simple tools like thought records or the Cognitive Triangle to help you start recognizing patterns. Most people spend 10-15 minutes each day reflecting or completing brief exercises between sessions. This approach is ideal for those who are ready to begin mapping their anxiety and celebrate even small changes in thinking or behavior. Research shows that these early steps lay the groundwork for meaningful symptom improvement over time6.
How do I choose between individual cognitive behavioral therapy for anxiety and group-based formats?
Choosing between individual and group-based cognitive behavioral therapy for anxiety depends on your clinical goals, comfort level, and the needs of those you serve. Individual CBT offers a highly personalized approach, tailored to each client’s unique anxiety triggers and pace. This path makes sense when privacy, focused attention, or complex dual diagnoses are top priorities. Group CBT, on the other hand, provides peer support, shared experiences, and opportunities to practice social skills in a safe setting. Consider this route if clients benefit from connection, normalization, and learning from others’ perspectives. Both formats are evidence-based and can deliver strong outcomes for anxiety disorders6.
Can cognitive behavioral therapy for anxiety work effectively alongside medication management?
Yes, cognitive behavioral therapy for anxiety can work effectively alongside medication management—many clients benefit from this integrated approach. Research suggests combined treatment often leads to greater symptom reduction than either option alone, especially in moderate to severe cases6. For example, pairing CBT with selective serotonin reuptake inhibitors (SSRIs) may help stabilize mood and provide the cognitive clarity needed to fully engage in therapy. This method suits individuals who have not achieved full remission with therapy or medication by itself, or those struggling with co-occurring conditions. Collaboration between prescribers and therapists is key, and regular communication helps you tailor treatment as symptoms shift. Remember, every bit of progress—no matter how small—counts on this journey.
What happens if I don’t respond to cognitive behavioral therapy for anxiety after several sessions?
If you don’t notice improvement from cognitive behavioral therapy for anxiety after several sessions, it’s understandable to feel discouraged, but it doesn’t mean you’ve failed or that change isn’t possible. About 20-30% of people may show limited response initially6. Sometimes, you and your therapist may need to adjust the treatment approach—this could involve reviewing goals, shifting techniques, or exploring co-occurring factors like trauma or medication needs. This approach works best when you remain open to feedback and collaborative problem-solving. Remember, progress can take time, and every attempt to refine your plan is a step forward. If needed, consider seeking a second opinion or integrated care for additional support.
How do digital cognitive behavioral therapy for anxiety programs compare to in-person treatment outcomes?
Digital cognitive behavioral therapy for anxiety programs are showing outcomes comparable to, and sometimes better than, traditional in-person treatment. For example, one study found that 71% of adults with generalized anxiety disorder achieved remission with smartphone-based CBT, compared to only 34.6% with psychoeducation alone9. These digital options make therapy more accessible for people facing barriers like transportation, scheduling, or stigma. This approach is ideal if your clients benefit from flexibility or need support outside of standard office hours. Yes, adapting to new formats can be challenging, but each completed digital module is a real step toward recovery.
Is cognitive behavioral therapy for anxiety effective when treating multiple co-occurring conditions simultaneously?
Absolutely—cognitive behavioral therapy for anxiety is effective when treating multiple co-occurring conditions at the same time. Research highlights that transdiagnostic CBT protocols can target shared patterns like avoidance, rigid thinking, and emotional dysregulation across anxiety, depression, and substance use disorders7. This method is especially useful if your clients present with overlapping symptoms or complex dual diagnoses, as it avoids fragmented care and supports skill generalization. You’ll typically need to coordinate with other providers and invest extra time in assessment and planning, but each integrated session helps your clients move forward. Celebrate each step—progress in even one area can spark positive change in others.
Your Next 30 Days: Implementation Pathway
You’ve made it this far, and that deserves recognition. The next 30 days can shape your dual diagnosis treatment journey in meaningful ways. Here’s a practical pathway to move forward with integrated care that addresses both your mental health and substance use needs simultaneously.
| Timeline | Focus Area | Key Actions |
|---|---|---|
| Week 1 | Stabilization | Establish safety, begin medication management, and start building therapeutic relationships. Participate in Partial Hospitalization programming to create a foundation. |
| Weeks 2-3 | Skill Development | Engage in individual and group therapy. Practice concrete tools like identifying triggers and developing distress tolerance skills for cravings and anxiety. |
| Week 4 | Integration | Apply new skills in daily life while maintaining structured support through Intensive Outpatient programming. Manage real-world challenges and adjust the plan as needed. |
This dual diagnosis treatment pathway isn’t rigid—your care adapts to you. Some days will feel harder than others, and that’s completely normal in dual diagnosis treatment. Progress isn’t linear, but with consistent effort and professional support through comprehensive dual diagnosis treatment, meaningful change happens. Every step forward in your dual diagnosis treatment journey counts, even the small ones.
References
- NIMH | Anxiety Disorders. https://www.nimh.nih.gov/health/topics/anxiety-disorders
- American Psychological Association | Understanding Anxiety. https://www.apa.org/science/about/psa/anxiety/understanding
- American Psychological Association | What Is Exposure Therapy?. https://www.apa.org/ptsd-guideline/patients-and-families/exposure-therapy
- CDC | Mental Health Treatment and Services. https://www.cdc.gov/mentalhealth/treatment-finding.html
- VA | PTSD: National Center for PTSD. https://www.va.gov/MENTALHEALTH/ptsd-overview.asp
- StatPearls | Cognitive Behavioral Therapy (Peer-Reviewed Medical Education). https://www.ncbi.nlm.nih.gov/books/NBK470361/
- SAMHSA | Find Treatment. https://www.samhsa.gov/find-help/treatment
- NAMI | About Mental Illness and Mental Health. https://www.nami.org/Get-Involved/Awareness-Events/Mental-Health-Awareness-Month/About-Mental-Health-Illness
- Psychology Today | Cognitive Behavioral Therapy (CBT). https://www.psychologytoday.com/us/basics/cognitive-behavioral-therapy
- Anxiety and Depression Association of America | Understanding Anxiety. https://adaa.org/understanding-anxiety



