Key Takeaways
- The first 30 days hinge on three sequenced decisions: honest screening with a validated tool, a withdrawal safety plan matched to medical risk, and a level of care that treats mental health alongside drinking.
- Severity is a spectrum, and NIAAA notes most people with AUD can benefit from some form of treatment, so waiting until things look bad enough is the wrong filter 7.
- Three non-addictive medications — acamprosate, naltrexone, and disulfiram — are approved for AUD and remain under-prescribed, making it fair to ask a prescriber whether one fits your plan 6, 3.
- Co-occurring mental health conditions should be treated concurrently, not sequentially, with one integrated team handling both the drinking and conditions like anxiety, PTSD, bipolar disorder, or ADHD 10.
The First 30 Days: Three Decisions That Shape Everything
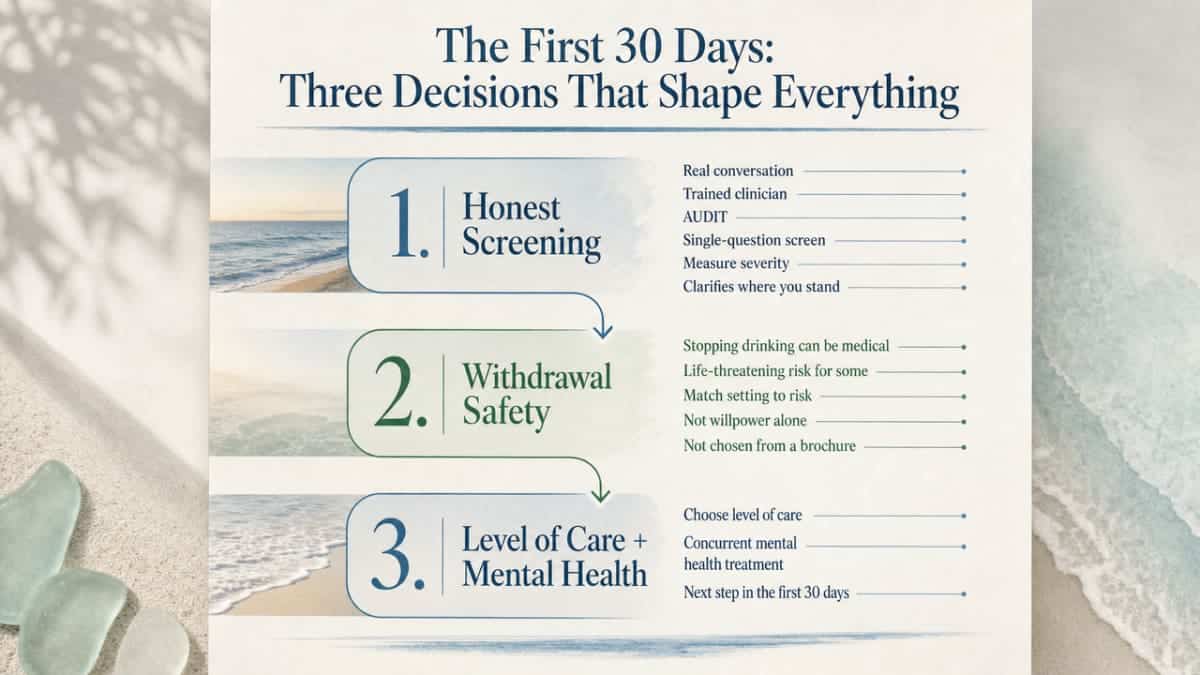
If you are reading this, something has already shifted. Whatever brought you here, the first 30 days of alcohol addiction treatment are less about finding the perfect program and more about making three decisions in the right order.
The first decision is honest screening. Not a quiz you took at 2 a.m., but a real conversation with someone trained to measure severity using tools like the AUDIT or a single-question screen 1. That conversation tells you where you actually stand, which changes everything that comes next.
The second decision is withdrawal safety. Stopping drinking is not always a willpower question. For some people, it is a medical one. Alcohol withdrawal can be life-threatening, and the setting where you go through it should be matched to your risk, not picked from a brochure 9.
The third decision is the level of care, chosen with your mental health in the same frame. If you live with anxiety, depression, PTSD, bipolar disorder, ADHD, OCD, or a personality disorder alongside your drinking, those conditions need to be treated at the same time, not after 10.
Get these three right, and the rest of alcohol addiction treatment has somewhere solid to begin.
Honest Screening: How Severity Actually Gets Measured
The Questions a Clinician Will Ask
A real screening conversation is shorter and gentler than you might expect. It usually starts with a validated tool, not a lecture. The most common is the AUDIT, a 10-question screen that asks about how often you drink, how much, and what has happened because of it. Some clinicians open with an even simpler single-question screen, like asking how many times in the past year you have had four or five drinks in a day 1.
From there, the questions get more specific. Have you tried to cut back and not been able to? Do you drink more or longer than you meant to? Has alcohol shown up in places it shouldn’t, like work, sleep, your relationships, your health? These are the markers SAMHSA names as signs that professional alcohol addiction treatment is worth considering 5.
A good clinician will also ask about your mental health in the same breath. Anxiety, depression, trauma, mood swings, attention struggles. Not as a side question, but because the answers shape what alcohol addiction treatment should look like for you.
This is what the research calls a brief intervention: feedback on risk, plain advice, a read on your readiness to change, a negotiated goal, and a follow-up plan 4. It is a conversation, not a verdict.
Why ‘I’m Not Sure I’m Bad Enough’ Is the Wrong Filter
One of the most common reasons people delay alcohol addiction treatment is a quiet thought: I’m not sure I’m bad enough yet. You still go to work. You haven’t lost anything obvious. You don’t drink in the morning. So maybe this isn’t the moment.
Here is what that filter misses. AUD lives on a spectrum, from mild to severe, and the science is clear that you do not have to hit a worst-case version of it to benefit from help. NIAAA puts it plainly: no matter how severe the problem may seem, most people with AUD can benefit from some form of treatment 7. Mild does not mean ignore. Mild means there is more room to work with, not less.
If you are also living with anxiety, depression, PTSD, bipolar disorder, ADHD, OCD, or a personality disorder, the math shifts again. Drinking and mental health feed each other in ways that make severity hard to judge from the inside. A screening conversation gives you an outside read, which is something a 2 a.m. self-assessment cannot do.
Making the appointment counts. Showing up counts. You do not have to be certain you belong in alcohol addiction treatment to start the conversation that tells you.
Withdrawal Triage: A Safety Decision, Not a Preference
Here is the part of alcohol addiction treatment that gets the least airtime and matters the most in week one: where you go through withdrawal is a medical call, not a comfort call. Alcohol withdrawal can be life-threatening, and the setting where it happens should be matched to your risk using structured clinical criteria, not picked because one option sounds less disruptive than another 9.
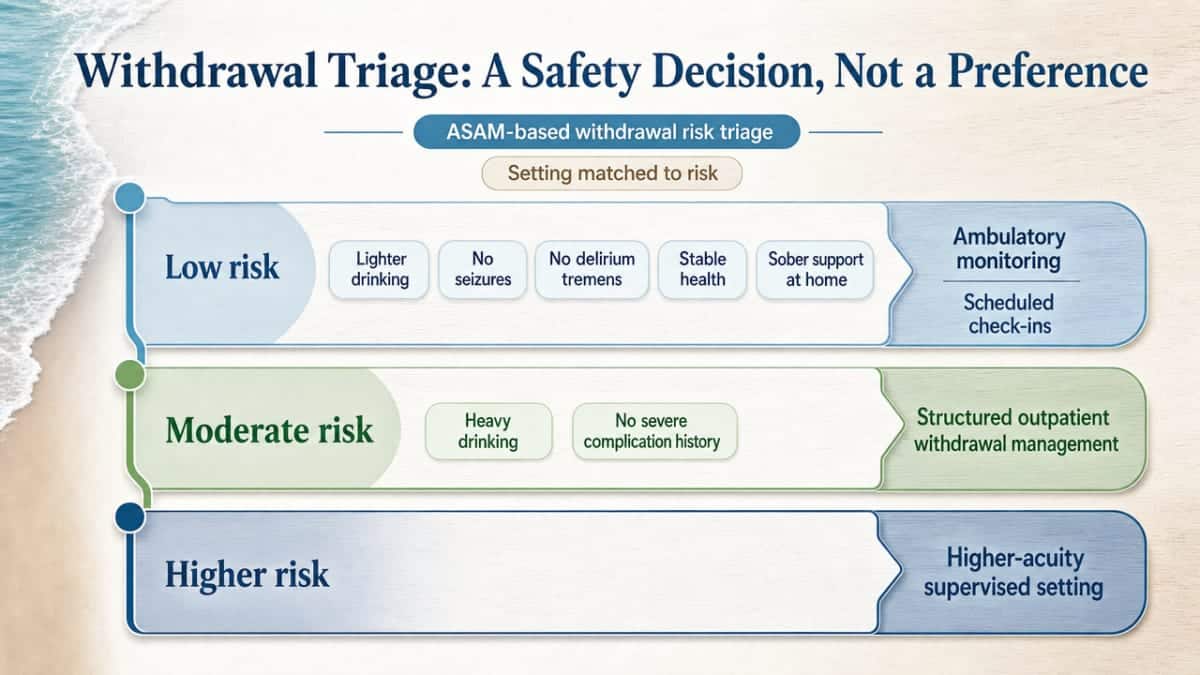
The ASAM guideline used by most clinicians sorts people into three broad paths:
- Low-risk withdrawal, meaning lighter drinking patterns, no history of seizures or delirium tremens, stable health, and a sober support person at home, can often be managed with ambulatory monitoring and scheduled check-ins.
- Moderate risk, where you drink heavily but have no severe complications in your history, usually points toward structured outpatient withdrawal management with medical oversight, daily vitals, and a clear medication plan.
- High risk, which includes a history of withdrawal seizures, delirium tremens, heavy daily drinking over a long stretch, serious medical conditions, or co-occurring mental health crises, calls for medically supervised withdrawal in a residential or hospital setting 9.
You do not assign yourself a category. A clinician does, using your drinking history, prior withdrawal experiences, current symptoms, vitals, and the realities of your home environment. That last piece matters. Even a moderate-risk profile can shift if you live alone, if there is alcohol in the house, or if your mental health is in a hard place right now.
If you have ever had a seizure when cutting back, seen things that were not there, or been told you experienced DTs, that history changes the math. Tell the person doing your assessment, even if it feels small or far away. It is the single most important thing they need to know before you stop drinking.
A note for anyone trying to white-knuckle through this at home: stopping cold without a plan is the most dangerous version of starting alcohol addiction treatment. Withdrawal symptoms often peak between 24 and 72 hours after the last drink, and the severe complications, including seizures and delirium tremens, can appear without much warning. If you are drinking daily and heavily, talk to someone before you stop. A primary care visit, a call to a treatment line, or a same-day evaluation at an outpatient program can sort out the safe path in a single conversation.
Matching Care Level to Real Life
Outpatient, Evening IOP, PHP, and Residential, Without the Jargon
The old framing of alcohol addiction treatment as a choice between rehab and outpatient leaves out most of what actually exists. Care happens on a ladder, and the right rung depends on how much structure you need to stay safe and make progress, not on how dramatic the label sounds.
Standard outpatient is the lightest level. You meet with a therapist and sometimes a prescriber one to a few hours a week, usually after work or school. It fits people who have completed a more intensive phase, or whose drinking and mental health symptoms are stable enough to work on with regular check-ins.
Intensive outpatient, or IOP, steps up to about nine to fifteen hours a week of group and individual sessions. Evening IOP is the version built for people who cannot stop working, parenting, or caregiving to enter alcohol addiction treatment. You keep your day. You spend your evenings doing real clinical work.
Partial hospitalization, or PHP, is the most structured form of outpatient care, typically five to six hours a day, several days a week. It looks a lot like a job. You go home at night. PHP is often the right starting point after withdrawal, especially when mental health symptoms are active.
Residential care means living onsite for a stretch of weeks. It is the right call when the home environment is unsafe, when prior outpatient attempts have not held, or when severe co-occurring symptoms need round-the-clock support.
NIAAA puts it this way: behavioral healthcare and AUD medications are about equally effective, and outcomes improve when clinicians offer a full menu of options and tailor the plan to the person 8. The level of care is part of that menu, not a verdict on how serious your situation is.
Working Adults, Caregivers, and What ‘Tailored Care’ Really Means
If you are holding down a job, raising kids, looking after a parent, or all three, you may have already decided alcohol addiction treatment is not realistic. It is. The structure just has to bend toward your life instead of the other way around.
Evening IOP exists for exactly this reason. So does the practice of layering PHP at the start of care and stepping down to IOP and then standard outpatient as you stabilize. The TIPs guidance from SAMHSA emphasizes person-centered care that adjusts intensity over time, including how mental health treatment is woven in at each step 10.
Tailored care also means the clinical plan reflects who you are outside the room. A night-shift nurse needs a different schedule than a parent of young kids. Someone with PTSD needs trauma-informed group settings, not just any group. A person managing bipolar disorder needs prescriber access that does not disappear when the program ends.
One conversation with an intake clinician usually sorts out which level fits this week. It can change next month. That is the design, not a failure of planning.
Medications for Alcohol Use Disorder: The Conversation Most People Never Have
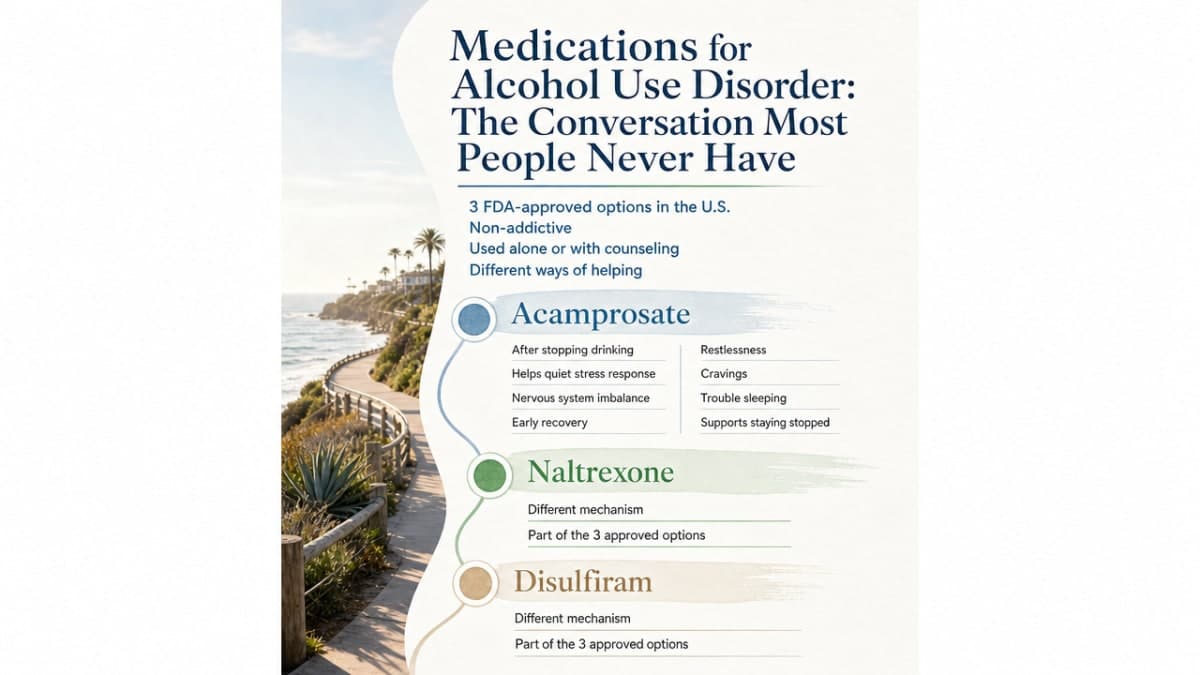
Here is something most people are never told when they start looking into alcohol addiction treatment: there are three medications approved in the United States for alcohol use disorder, and all three are non-addictive. They can be used alone or alongside counseling, and they exist precisely because willpower is not the variable that decides who gets better 6.
The three are acamprosate, naltrexone, and disulfiram. Each works in a different way.
Acamprosate helps quiet the brain’s stress response after you stop drinking. Heavy alcohol use changes how the nervous system regulates itself, and acamprosate works on that imbalance so the noise of early recovery — the restlessness, the cravings, the trouble sleeping — gets quieter. It is most often used once you have already stopped drinking and want to stay stopped 6.
Naltrexone takes a different angle. It blocks the receptors that make drinking feel rewarding, so a drink does not deliver the same hit it used to. People taking naltrexone often describe a kind of flatness around alcohol — they can take it or leave it, and leaving it gets easier. It comes as a daily pill or as an extended-release injection given once a month, which removes the daily decision entirely 6. The extended-release form is one of the more useful recent additions to alcohol addiction treatment for people who struggle with the day-to-day reminder of taking a pill.
Disulfiram is the oldest of the three and works by deterrence. If you drink while taking it, you get sick — nausea, flushing, headache. For some people, knowing that the option is off the table is exactly the structure they need. It works best with daily supervision or strong external support 3.
None of these medications cure alcohol use disorder. They are tools that lower the intensity of the fight, so the work you do in therapy and in your daily life has a better chance of landing. SAMHSA is direct about the pairing: these medications are most effective when combined with counseling 6.
If you live with a mental health condition alongside your drinking, the medication conversation gets more layered, not less worth having. A prescriber who understands dual diagnosis can coordinate AUD medications with what you take for anxiety, depression, bipolar disorder, or PTSD, so the plan holds together instead of competing with itself.
One last thing worth saying plainly. AUD medications are under-prescribed relative to what the evidence supports, which means many people who would benefit from them never get the offer 3, 8. If you start alcohol addiction treatment and no one brings up medication, you can bring it up. Asking, “Would a medication for AUD make sense for me?” is a fair and useful question. The answer might be yes, no, or not yet — but the conversation itself belongs on the table from the start of alcohol addiction treatment, not as an afterthought months in.
Treating Mental Health and Alcohol Use at the Same Time
Why Sequential Care Fails Dual Diagnosis
For a long time, the standard advice for someone with both a mental health condition and a drinking problem went something like this: get sober first, then we’ll deal with the depression. Or, stabilize the bipolar disorder first, then we’ll address the alcohol. That order sounds reasonable on paper. In practice, it leaves people stuck in a loop that rarely breaks on its own.
Here is why. If you are drinking to quiet panic attacks, intrusive memories, or the static of untreated ADHD, asking you to stop drinking before treating the underlying condition removes the only coping tool you have, without replacing it. The mental health symptoms get louder, the cravings get sharper, and the relapse that follows gets read as a willpower failure instead of a design flaw in the plan.
SAMHSA’s TIPs guidance is direct about this. Co-occurring mental health conditions should be addressed concurrently rather than sequentially in alcohol addiction treatment 10. That single shift — concurrent instead of stacked — is what separates dual diagnosis care from generic rehab with a therapist bolted on.
If you have ever been told to come back for alcohol addiction treatment once your mental health was stable, or to come back for mental health care once you were sober, you were not failing the system. The system was failing you.
What Integrated Treatment Looks Like Week to Week
Integrated care is less exotic than it sounds. It means one team, one treatment plan, and both conditions in the same room at the same time.
In practice, a week of integrated alcohol addiction treatment might include individual therapy that moves between your drinking patterns and your trauma history without forcing you to pick a lane. A psychiatric appointment where the prescriber considers your AUD medication and your antidepressant or mood stabilizer as one prescription puzzle, not two. Group sessions where the people next to you are also working both sides — anxiety and drinking, PTSD and drinking, bipolar disorder and drinking — so you are not the only one translating.
The therapies do double duty. Cognitive behavioral therapy targets the thought patterns that drive both drinking and depression. Dialectical behavior therapy gives you skills for the emotional intensity behind both substance use and personality disorder symptoms. Trauma-focused work, including EMDR, addresses the source of what you have been numbing.
Programs that specialize in dual diagnosis, including outpatient settings like PHP and evening IOP, are built around this design. The level of care flexes. The integration does not. That is the part that makes alcohol addiction treatment hold when life gets hard again, which it will.
Therapies That Actually Do the Work
Behind every successful alcohol addiction treatment plan is a small set of therapies that have earned their place through evidence, not marketing. You do not need to learn the acronyms before you walk in. You will pick them up. But knowing what to expect makes the first sessions less intimidating.
Cognitive behavioral therapy teaches you to spot the thoughts that lead to drinking and rework them in real time. It is practical, skill-based, and well-suited to people who also live with depression or anxiety 8.
Motivational interviewing meets you where your ambivalence actually sits. Instead of arguing you into change, a clinician helps you talk through your own reasons, which tends to stick longer 8.
Dialectical behavior therapy builds skills for tolerating distress, regulating emotions, and staying steady in relationships. It is the standard of care for personality disorder symptoms and pulls double duty in alcohol addiction treatment when emotional intensity drives the drinking.
Trauma-focused therapies, including EMDR, address the memories and responses that many people have been numbing for years. Doing this work alongside alcohol addiction treatment, not after, is what the dual diagnosis evidence supports 10.
Mutual support groups, including 12-step and alternatives, round out the picture for many people. NIAAA names them as part of a full menu of options worth offering 8. Pick what fits. You can add or drop along the way.
Making the First Call and What Happens After
The hardest part of alcohol addiction treatment is often the part nobody clinical can do for you: picking up the phone. Not the therapy, not the medication conversation, not the withdrawal plan. The call.
Here is what helps. You do not need a script. You do not need to know whether you want IOP or PHP, naltrexone or acamprosate, weekly or daily. You need one sentence: “I’m trying to figure out what to do about my drinking, and I think there’s also some mental health stuff going on.” That is enough. The person on the other end is trained to take it from there.
SAMHSA runs a free, confidential helpline at 1-800-662-HELP, available 24 hours a day in English and Spanish, that connects callers to local alcohol addiction treatment options 11. If you would rather start with a clinic directly, an intake call usually takes 15 to 30 minutes. You answer some questions about your drinking, your mental health, your medical history, and your schedule. They tell you what a first appointment would look like and when they can see you.
The first appointment itself is mostly listening on their end. A clinician walks through a structured assessment, talks with you about withdrawal risk, and starts mapping a care plan. You will leave with a next step, not a finished plan. That is the right pace.
One call. One appointment. One honest conversation. That is how alcohol addiction treatment actually starts.
Frequently Asked Questions
How do I know if my drinking is bad enough to need alcohol addiction treatment?
If you are asking the question, that is already a useful signal. You do not need to hit a worst-case version of drinking to benefit. NIAAA is clear that most people with AUD can benefit from some form of treatment, regardless of severity 7. A short screening conversation with a clinician will tell you where you actually stand and what level of care, if any, fits.
Is alcohol withdrawal really dangerous, or can I just stop drinking on my own?
Alcohol withdrawal can be life-threatening, especially if you drink heavily and daily or have a history of seizures or delirium tremens 9. Stopping cold without a plan is the riskiest version of starting alcohol addiction treatment. A clinician can match the setting — ambulatory monitoring, structured outpatient, or medically supervised withdrawal — to your risk in a single assessment. Talk to someone before you stop.
What medications are approved for alcohol use disorder, and are they addictive?
Three medications are approved in the United States for AUD: acamprosate, naltrexone (including a once-monthly extended-release injection), and disulfiram. All three are non-addictive and may be used alone or alongside counseling 6. They are under-prescribed relative to the evidence, so if no one brings them up during your alcohol addiction treatment, it is fair to ask whether a medication makes sense for you 3.
Should I treat my mental health condition first, or my drinking first?
Neither first. SAMHSA’s guidance is that co-occurring mental health conditions should be addressed concurrently rather than sequentially in alcohol addiction treatment 10. If you have been told to get sober before therapy or to stabilize your mental health before rehab, that order has been shown to leave people stuck. Look for integrated care where one team handles both conditions in the same plan.
What is the difference between outpatient, IOP, PHP, and residential care?
They differ in hours per week and structure. Standard outpatient is a few hours weekly. Intensive outpatient (IOP), including evening IOP, runs about nine to fifteen hours. Partial hospitalization (PHP) is the most structured outpatient option, often five to six hours a day. Residential means living onsite. NIAAA recommends offering a full menu of options and tailoring care to the person, not picking by label 8.
What actually happens on the first call or first appointment?
The first call usually takes 15 to 30 minutes. Someone asks about your drinking, mental health, medical history, and schedule, then explains next steps. SAMHSA’s National Helpline (1-800-662-HELP) is free, confidential, and available 24/7 if you want a starting point 11. The first appointment is mostly listening on their end — a structured assessment and an early plan. You leave with a next step, not a finished plan.
References
- Screen and Assess: Use Quick, Effective Methods. https://www.niaaa.nih.gov/health-professionals-communities/core-resource-on-alcohol/screen-and-assess-use-quick-effective-methods
- Screening and Behavioral Counseling Interventions in Primary Care to Reduce Unhealthy Alcohol Use in Adults. https://www.ahrq.gov/prevention/guidelines/guide/section3c.html
- Pharmacotherapy for adults with alcohol use disorders in outpatient settings: A review. https://pubmed.ncbi.nlm.nih.gov/35290155/
- Chapter 3—Brief Intervention – A Guide to Substance Abuse Services for Primary Care Clinicians. https://www.ncbi.nlm.nih.gov/books/NBK64821/
- Alcohol Use Disorder: Causes, Symptoms, Treatment & Help. https://www.samhsa.gov/substance-use/learn/alcohol
- Treatment Options for Substance Use Disorder. https://www.samhsa.gov/substance-use/treatment/options
- Treatment for Alcohol Problems: Finding and Getting Help. https://www.niaaa.nih.gov/publications/brochures-and-fact-sheets/treatment-alcohol-problems-finding-and-getting-help
- Recommend Evidence-Based Treatment: Know the Options. https://www.niaaa.nih.gov/health-professionals-communities/core-resource-on-alcohol/recommend-evidence-based-treatment-know-options
- The ASAM Clinical Practice Guideline on Alcohol Withdrawal Management: Pocket Guide. https://www.samhsa.gov/resource/ebp/asam-clinical-practice-guideline-alcohol-withdrawal-management-pocket-guide
- Substance Abuse Treatment: Treatment Improvement Protocols (TIPs). https://www.ncbi.nlm.nih.gov/books/NBK82999/
- National Helpline for Mental Health, Drug, Alcohol Issues. https://www.samhsa.gov/find-help/helplines/national-helpline



