
Key Takeaways
- Regulatory Rights: California’s Mental Health Parity Act ensures your insurance covers mental health treatment CA at the same level as physical health services, including out-of-network protections.
- Regional Access: Availability of care varies significantly, with distinct differences between urban hubs like Los Angeles and the Bay Area versus the Central Valley and rural northern counties.
- Workforce Reality: The state faces a projected 42% shortfall in clinicians by 2033, impacting wait times and access to specialized dual diagnosis care.
- State Resources: The Department of Health Care Services (DHCS) oversees licensing and compliance to ensure safety and quality standards across all counties.
California’s Behavioral Health Landscape
Workforce Crisis & System Strain
When you look at California’s behavioral health system, finding effective mental health treatment CA can feel like navigating a maze, especially given the mounting strain caused by an escalating workforce crisis. From the Bay Area to the Central Valley and the Inland Empire, the shortage of licensed mental health professionals impacts every region, with rural counties like those in the northern part of the state hit especially hard. By 2033, California faces a projected shortfall of 42% in nonprescribing licensed behavioral health clinicians, meaning nearly double the current workforce will be needed to meet demand3.
Even now, some residents endure hours-long drives for essential detox or psychiatric services, particularly in the state’s far north and agricultural regions2. This strain does more than slow access—it increases wait times, stretches existing teams thin, and amplifies burnout among dedicated clinicians. Yes, it’s tough, and every effort you make to support integrated care truly matters. The crisis isn’t limited to one population or location; all 58 counties are expected to feel the impact, with urban hubs like Los Angeles and San Diego also reporting gaps in psychiatry coverage3. As you adapt to these realities in mental health treatment CA, know that your resilience and commitment are part of what keeps the system moving forward.
Prevalence & Population Impact
California’s behavioral health needs run deep and wide, touching every corner of the state—from the urban sprawl of Los Angeles and San Diego to the Central Valley and even the rural North Coast. An estimated 5.6 million Californians aged 12 and older—about 17% of the state’s population—met criteria for a substance use disorder between 2022 and 20231. At the same time, rates of anxiety, depression, and suicidal ideation remain high across age groups and backgrounds.

For example, 35% of LGBTQ+ young people in California reported seriously considering suicide in the past year8.
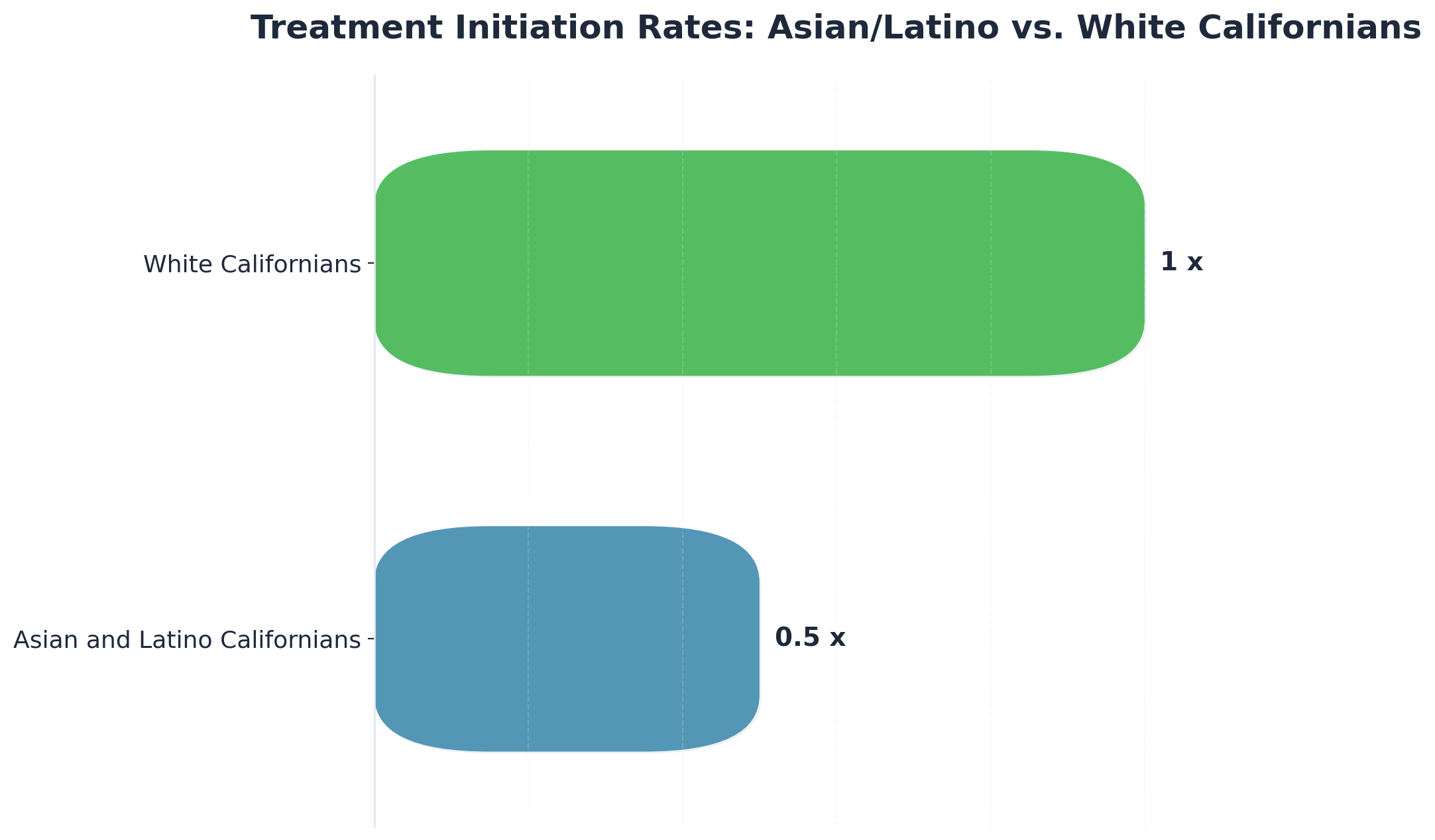
These numbers aren’t just statistics—they represent real people and families navigating the challenges of mental health treatment CA. Disparities make the journey even tougher: Asian and Latino Californians are half as likely as White Californians to initiate care, and Black Californians often face double the wait times for step-down services6. Each region has its own challenges; the Inland Empire and Central Valley continue to report some of the lowest treatment initiation rates, while the Bay Area struggles with access for non-English speakers and marginalized groups. Yes, the obstacles are real, but even a small increase in access or engagement means progress.
State Regulations & Standards for Mental Health Treatment CA
Licensing Requirements & DHCS Oversight
Licensing in California is a formidable hurdle, but it’s also the backbone of public trust and safety for mental health treatment CA. The Department of Health Care Services (DHCS) is the primary regulator overseeing the licensure, certification, and monitoring of outpatient, residential, and detox facilities statewide. Whether you’re serving clients in Los Angeles, San Diego, or up in the Shasta County region, you’re expected to meet rigorous standards for clinical staffing, documentation, and safety protocols, which include compliance with Title 9 regulations and DHCS bulletins.
To operate legally, programs must hold a current DHCS license. This includes strict background checks, regular inspections, and demonstration of evidence-based practices tailored to California’s diverse population. Outpatient programs, especially those offering integrated dual diagnosis services, are also required to adhere to Medi-Cal billing protocols, which can be a maze of state-specific codes and utilization review processes5. Yes, these details can be overwhelming, and it’s completely normal to feel stretched—especially when regulations evolve faster than your team can update procedures.
DHCS oversight isn’t just about rules; it’s about ensuring equity. The agency actively audits programs for culturally competent care, language access, and proper service delivery in communities from the Bay Area to the Central Valley5. Every adjustment you make toward compliance is a win—progress matters.
Mental Health Parity Implementation
California’s Mental Health Parity Act stands as one of the strongest state-level protections for behavioral health coverage, but real-world implementation can still trip up even the most dedicated teams. Since being expanded in 2020, the law requires all state-regulated commercial health plans to cover every mental health and substance use disorder listed in the DSM or ICD—no more limiting coverage to only a few severe diagnoses5. If you can’t find an in-network provider in your area, the plan must pay for out-of-network care at in-network rates, a safeguard that’s especially critical in underserved regions like the Central Valley and the far north.
On paper, these rules should make mental health treatment CA accessible to millions, but actual enforcement remains uneven. State investigations have found major insurance networks in Los Angeles, the Bay Area, and San Diego out of compliance—patients have faced long waits and improper denials, particularly for dual diagnosis or step-down outpatient care5. As a professional, you know how exhausting it is to advocate for coverage while managing clinical needs. Every successful appeal, every client who gets approved after an initial denial, is a meaningful win.
Evidence-Based Modalities in Mental Health Treatment CA
Integrated Dual Diagnosis Approaches
Integrated dual diagnosis approaches have become the foundation of mental health treatment CA for individuals with co-occurring substance use and mental health disorders. In California, you know firsthand how siloed systems used to leave significant gaps—especially for clients navigating both addiction and complex psychiatric needs. The state has responded by actively promoting integrated models, where substance use and mental health are addressed together, not in isolation.
For example, the Drug Medi-Cal Organized Delivery System (DMC-ODS) now covers 96% of the state’s Medi-Cal population, creating a pathway for coordinated, evidence-based care1. Regions like Los Angeles and the Bay Area have led in building multidisciplinary teams—combining psychiatry, addiction medicine, case management, and peer support—helping clients achieve better engagement and reduced relapse rates. This approach is especially critical in counties with high rates of dual diagnosis, as seen in Central Valley communities where up to 17% of residents meet criteria for a substance use disorder1.
California’s regulatory framework also supports these models, requiring programs to deliver culturally responsive, trauma-informed, and person-centered care. The push for integration has led to the adoption of therapies like Cognitive Behavioral Therapy (CBT), Motivational Interviewing, and medication-assisted treatment within the same outpatient settings, even in more rural areas. Yes, the work is demanding, but every time a client finds stability through this comprehensive approach, it’s a win worth celebrating.
Trauma-Informed & Dialectical Frameworks
Trauma-informed and dialectical frameworks aren’t just buzzwords in mental health treatment CA—they’re essential, evidence-based approaches that have taken root statewide, especially in response to the high prevalence of trauma and complex co-occurring conditions. Whether you’re practicing in the Bay Area, Los Angeles, or up in the North State, you’ve likely seen firsthand how trauma shapes clinical needs and engagement.
California’s regulatory landscape encourages trauma-informed care, requiring programs to recognize the effects of adverse experiences and build safety, trust, and empowerment into every level of service delivery. That’s not just policy—it’s real change, especially for communities with high rates of historical and intergenerational trauma, such as Black, Indigenous, and LGBTQ+ Californians, who are overrepresented in crisis episodes and system involvement6, 8.
Dialectical Behavior Therapy (DBT), in particular, has gained traction for treating severe emotion dysregulation, personality disorders, and suicidality. Several counties—including Orange County and Sacramento—have adopted DBT as a standard in their outpatient and crisis programs, with measurable improvements in treatment retention and reduced self-harm incidents8. Therapies like EMDR are also being woven into trauma-focused groups, reflecting the state’s commitment to integrated, culturally responsive modalities.
Regional Considerations & Access Disparities
If you’re searching for dual diagnosis treatment in California, you’ve probably already discovered what many people facing co-occurring disorders experience: access to comprehensive care varies dramatically depending on where you live. Urban centers like Los Angeles, San Diego, and the San Francisco Bay Area typically offer more specialized treatment options, while rural and inland communities often have significant gaps in care. If you’re in a less-populated area, you might feel frustrated by limited local options—and that’s completely understandable. These geographic inequalities create real challenges when you need immediate, comprehensive support for simultaneous mental health and substance use issues.
| Region | Service Availability | Common Challenges |
|---|---|---|
| Southern California (Orange County, LA, San Diego) | High concentration of specialized IOP/PHP, DBT programs, and integrated dual diagnosis centers. | Network bottlenecks, high cost of living affecting provider availability, and variable insurance acceptance. |
| Northern California (Rural Counties, North Coast) | Limited local options for unified dual diagnosis approaches; often requires travel for specialized care. | Significant workforce shortages, long travel times, and fewer providers offering integrated mental health treatment CA. |
Transportation barriers can make these access issues even more challenging. If you don’t have reliable transportation or public transit options in your area, maintaining consistent participation in Partial Hospitalization Programs or Intensive Outpatient Programs can feel nearly impossible. Missing sessions creates gaps in your care, which can affect your therapeutic progress and increase relapse risk—and you deserve better than that.
Insurance network limitations create another layer of complexity you might be navigating right now. While major commercial insurers increasingly cover coordinated services for dual diagnosis conditions, network adequacy varies by region. Some areas have robust in-network provider options, while others leave you with few choices or require out-of-network care that creates financial barriers you shouldn’t have to face alone. Evening IOP offerings help address some of these access challenges by accommodating work schedules, though availability remains inconsistent across regions.
Proposition 1 & California’s Infrastructure Investment
There’s good news for your recovery journey—California just made a major investment in exactly the kind of comprehensive care you need. In March 2024, voters passed Proposition 1, a $6.38 billion commitment to mental health and substance use treatment that prioritizes integrated care. This means more facilities will offer the dual diagnosis treatment that addresses both your mental health and substance use challenges together, under one roof, with one coordinated team supporting you.
Here’s what this means for you and the future of mental health treatment CA:
- Integrated Funding: Proposition 1 directs significant funding toward outpatient programs that combine psychiatric care with substance use treatment—recognizing that when you’re dealing with both, you shouldn’t have to choose between them.
- Flexible Options: The infrastructure improvements prioritize flexible treatment options that fit into your life—programs like Partial Hospitalization and Intensive Outpatient services that provide comprehensive care while allowing you to maintain your job and family responsibilities.
- Coordinated Teams: You’ll have access to evidence-based therapies, medication management when needed, and therapeutic support all coordinated through one treatment team who understands your complete picture.
If you’re in Orange County, these improvements mean enhanced access to quality dual diagnosis treatment right in your community. The funding flows to accredited facilities that meet rigorous standards and demonstrate real clinical effectiveness—places that combine psychiatric care, therapy, and addiction treatment through coordinated approaches designed specifically for people navigating both challenges. You’ll have more options for comprehensive care that treats all of you, not just parts of your experience.
Understanding how Proposition 1 shapes California’s treatment landscape helps you recognize the growing commitment to the kind of integrated care you deserve—and how these investments are expanding access to dual diagnosis treatment for people facing overlapping challenges just like yours. Help is becoming more available, and your recovery journey has more support than ever before.
Frequently Asked Questions
How does California’s Mental Health Parity Act affect out-of-network coverage?
California’s Mental Health Parity Act requires state-regulated health plans to cover all medically necessary mental health and substance use disorder services—just like physical health. If an in-network provider for mental health treatment CA isn’t available in your client’s region, the law mandates coverage for out-of-network care at the same in-network rate. This safeguard is especially crucial in places like the Central Valley and rural north where network adequacy is often an issue. While enforcement isn’t perfect and denials still happen, the parity law gives you a solid foundation to advocate for your clients and push insurers to honor their obligations5.
What role do peer support specialists play in California’s behavioral health system?
Peer support specialists are a driving force in California’s behavioral health system, offering lived experience and hope to people navigating recovery. Since the launch of the Medi-Cal Peer Support Specialist Certification, over 5,000 individuals have been certified to provide recovery-oriented services across the state9. You know how valuable this is—peers bring cultural understanding, reduce stigma, and help clients stay engaged, especially in communities where trust in traditional providers is low. Their work is now reimbursable through Medi-Cal, making it easier for programs in Los Angeles, the Bay Area, and the Central Valley to integrate peer support directly into mental health treatment CA. Every story shared and every connection built by a peer specialist is a win for recovery and engagement.
Why do wait times for mental health services vary so significantly across California counties?
Wait times for mental health services in California vary widely due to a mix of workforce shortages, uneven funding, and regional infrastructure gaps. Counties in the far north and Central Valley often have fewer licensed clinicians per resident, forcing some people to travel hours for care—while Bay Area or Los Angeles residents may have shorter waits but still face network bottlenecks26. Disparities are even sharper for Black, Asian, and Latino Californians, who may wait twice as long for step-down care or are half as likely to initiate treatment compared to White residents6. Every improvement—even a few days less waiting—means real progress toward equitable mental health treatment CA.
What is the 988 crisis line and how does it differ from traditional emergency services?
The 988 crisis line is California’s dedicated suicide and mental health crisis lifeline, launched statewide in July 2022 as a direct response to the need for urgent, culturally responsive support. Unlike 911, which often triggers a law enforcement or EMS response, 988 connects callers to trained crisis counselors at one of 12 local call centers based on area code. Over 90% of calls are resolved by phone, without police involvement, with mobile crisis teams available for higher-risk situations7. This approach helps de-escalate crises, prevent unnecessary ER visits or arrests, and offer rapid linkage to mental health treatment CA. Every call answered is a step toward safer, more compassionate care.
How will Proposition 1 funding specifically impact outpatient treatment capacity?
Proposition 1 is set to make a significant difference in outpatient treatment capacity across California. With $6.4 billion in funding, the state plans to add 26,700 new outpatient treatment slots—directly addressing the bottlenecks that often leave people waiting weeks for care in places like Los Angeles, the Bay Area, and the Central Valley. This expansion will help you provide quicker access to integrated, community-based mental health treatment CA, especially for individuals with complex needs or experiencing homelessness. Counties will have flexibility to tailor these new resources locally, ensuring that every region’s specific gaps are addressed4. Every new slot opened is a real win for access and equity.
What protections exist for non-English speakers accessing mental health services in California?
California law requires all state-licensed mental health programs and health plans to provide language access and interpreter services at no cost for non-English speakers seeking mental health treatment CA. This means clients in Los Angeles, the Bay Area, or the Central Valley have the right to receive information, consent forms, and treatment in their preferred language whenever possible56. Still, only about 1% of Californians whose primary language is Spanish, Cantonese, or Vietnamese engage with the specialty mental health system, compared to 3% of English speakers—highlighting ongoing barriers6. Every time you help a client overcome a language gap, you’re advancing equity and opening doors for more inclusive care.
How does California’s approach to medication-assisted treatment in correctional facilities compare to community standards?
California has made significant strides in providing medication-assisted treatment (MAT) for opioid use disorder within its correctional facilities, often exceeding community standards. As of late 2024, 60% of incarcerated individuals with an identified opioid use disorder in state prisons were actively receiving MAT—about double the most recent community estimates10. This is possible through the Integrated Substance Use Disorder Treatment (ISUDT) program, which ensures medications like buprenorphine and methadone are accessible inside correctional settings. While community access to MAT can still be inconsistent—especially in rural or under-resourced counties—California’s correctional facilities have become a model for rapid MAT scale-up and overdose prevention. Every person maintained on MAT inside or outside the system is a win for health equity and recovery-focused mental health treatment CA.
Accessing Integrated Care in Southern CA
Finding the right support for co-existing mental health and substance use challenges can feel overwhelming, especially when you’re navigating a crisis. You’re dealing with something complex, and it makes sense that figuring out where to turn feels difficult right now. Southern California has a strong network of facilities offering integrated dual diagnosis treatment—programs designed to address both conditions simultaneously, because treating one without the other rarely leads to lasting recovery.
You’ll find options ranging from partial hospitalization programs for intensive daily support to intensive outpatient programs that let you maintain work and family responsibilities while getting the care you need. When you’re ready to reach out, look for facilities that treat both conditions together—because you deserve care that sees the whole picture. You might start by calling your insurance to ask about in-network dual diagnosis programs, or reach out to a facility directly for a confidential assessment.
CARF-accredited and DHCS-licensed centers that specialize in concurrent disorders typically offer comprehensive assessments to understand your unique situation and create a personalized treatment plan. Many work with major insurance providers, which can make accessing quality mental health treatment CA more manageable. Taking this step—even just making that first phone call—matters more than you might realize right now.
References
- Substance Use in California Almanac — 2025 Edition. https://www.chcf.org/publication/substance-use-california-almanac-2025-edition/
- As California’s behavioral health workforce buckles, help is years away. https://www.latimes.com/california/story/2024-06-03/as-californias-behavioral-health-workforce-buckles-help-is-years-away
- Every California county to face clinician shortages by 2033. https://www.beckersbehavioralhealth.com/behavioral-health-workforce/every-california-county-to-face-clinician-shortages-by-2033.html
- Proposition 1 continues delivering support for vulnerable homeless populations. https://www.gov.ca.gov/2024/07/01/proposition-1-continues-delivering-support-for-vulnerable-homeless-populations/
- Behavioral Health Care – DMHC.ca.gov. https://www.dmhc.ca.gov/healthcareincalifornia/yourhealthcarerights/behavioralhealthcare.aspx
- Existing Disparities in California’s System of Specialty Mental Health Care. https://cpehn.org/sites/default/files/resource_files/cpehn_factsheet_mhdisparities_final.pdf
- 988 – California’s Crisis Care Continuum. https://www.chhs.ca.gov/988/
- 2024 Survey on the Mental Health of LGBTQ+ Young People in California. https://www.thetrevorproject.org/research/cadata-2024/
- Peer Certification. https://www.calmhsa.org/peer-certification/
- ISUDT 4th Annual Outcomes Report (May 2025). https://cchcs.ca.gov/wp-content/uploads/sites/60/2024/05/ISUDT-4th-Annual-Outcomes-Report-May-2024_A.pdf



